Our conversation is out as the February episode. Listen on Spotify/Apple or on Perspective 2020 Pod website.

Our conversation is out as the February episode. Listen on Spotify/Apple or on Perspective 2020 Pod website.
At the end of April, the dean of the University of Michigan School of Public Health and associate dean of education at UM SPH penned an op-ed regarding stacked best practices as Michigan and the country begin to allow certain businesses to operate again. Drs. Bowman and Kardia wrote: Our research tells us that stacking best practices—with several layers of safeguards to reduce the spread of COVID-19 and lower the risk of another spike in cases and deaths—is necessary to manage this outbreak while re-engaging our economy.
They make an analogy that stacked best practices like mask wearing, hand washing, sneeze guards for cashiers, split work time in cubicle settings are the same as the group of behaviors we engage in around driving: air bags, stop signs, speed limits. You can watch this video which further explains this analogy.
Esteemed physician and writer Dr. Atul Gawande also wrote about a regimen for re-entry. He similarly discusses the “combination therapy” we should embrace upon re-opening just as we use combination therapies for cancer. “Its elements are all familiar: hygiene measures, screening, distancing, and masks. Each has flaws. Skip one, and the treatment won’t work. But, when taken together, and taken seriously, they shut down the virus.”
An Assistant Professor at the Johns Hopkins University Center for Health Security, Dr. Caitlin Rivers, shared a Twitter thread with her thoughts on viral transmission in a more open world. “Our actions, the choices we make, are the front lines. We should stay home when we can, avoid gatherings, wear masks indoors in public, wash hands. This next phase is up to us, and it’s with continued vigilance that we can further slow the virus.”
Several pre-prints have modeled the impact that universal mask wearing can have on the pandemic. Eikenberry et al states, “Despite uncertainty, the potential for benefit, the lack of obvious harm, and the precautionary principle lead us to strongly recommend as close to universal (homemade, unless medical masks can be used without diverting healthcare supply) mask use by the general public as possible.” In Figure 1 of Howard et al we see at 80% adherence and 40% mask efficacy we would reduce the reproduction number to < 1 which is the goal to eventually end viral spread.
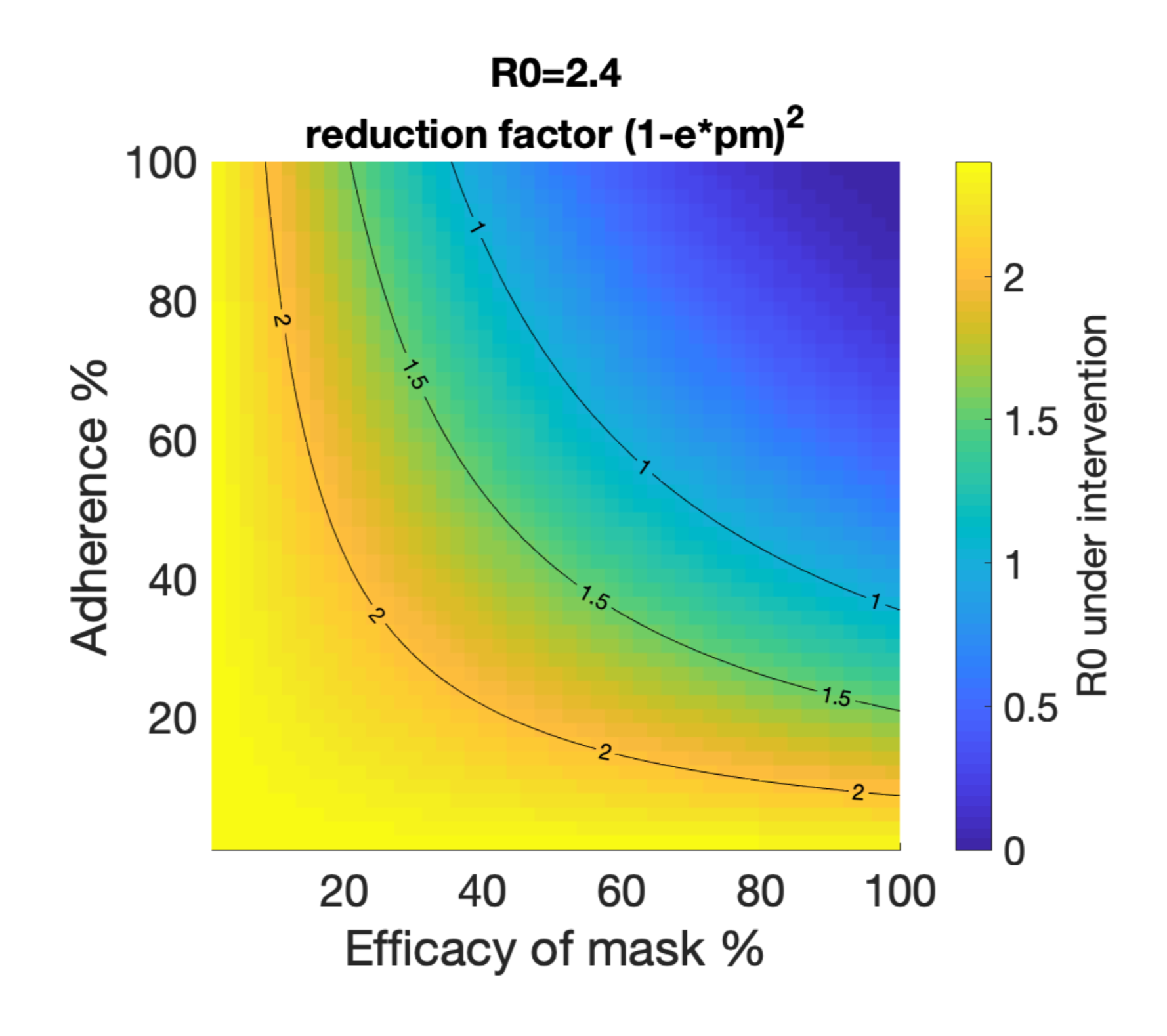
The impact of public mask wearing as modeled in a pre-print by Howard et al. We want to be in the blue.
The purpose of stacking best practices is holistic risk reduction. An epidemiologist at Boston University, Dr. Ellie Murray, suggests considering a COVID-19 contact budget. She and other scientists created an infographic on risk across a variety of settings. You can read more about what experts think of risks across settings here and here. Neurologist and science communicator, Dr. Samantha Yammine summarized a lot of risk reduction resources in an Instagram post. She points out the four dimensions of risk are distance, environment (indoors or outdoors), activity, and time. The two directions we have to consider are risk to our personal health and risk to others.
Public policy regarding public health is constantly evolving and sometimes contradictory, especially during an ongoing pandemic. For example, early messaging in the U.S. dissuaded mask usage, but now public policy strongly encourages or mandates masks. You can read more here. Understandably, this is frustrating for the general public. Because knowledge is power, I encourage you to follow the ever-changing public policy landscape as much as you are able. Contact your elected officials to voice your educated opinions too!
The Centers for Disease Control and Prevention (CDC) recently released a lengthy document supporting the President’s plan for re-opening the country. I’ll point you to page 7 which describes thresholds for entering various phases of re-opening. Many states have outlined similar phases. Page 45 has interim guidance for schools and day camps. The CDC also released interim guidance for communities of faith. Because the pandemic has different time lines and magnitudes across the U.S., I encourage you to check the information released by your county and state’s Public Health Departments. Many of these organizations have Facebook pages to communicate with the community.
A new data visualization tool allows simultaneous tracking of social distancing trends, policy decisions, and cumulated COVID-19 cases in the U.S. and in each state. I found this resource thanks to Andy Slavitt’s Twitter and it is hosted by the Surgo Foundation, a self-proclaimed “action tank” working to bring the latest innovations around behavior, tech, and data to global development (I say all this in the effort to consider biases and sources of conflict from the places we get our evidence, read my last post here). As responsible citizens, we have to keep an eye on the complex interplay of viral transmission, interpersonal behavior, and public policy!
If you’re still looking for information about the novel coronavirus, including what it does to lungs and how it infects cells, I suggest the Coronavirus Center at Lifeology. They have several illustrated stories to help kids understand the virus too!
There are a lot of epidemiologists, clinicians, and more sharing their expertise on Twitter. Dr. Angela Rasmussen created a list (made in response to an article highlighting just a few men, but the list stands alone as an incredible source outside of the issue of representation). Dr. Yammine also curated a list of key sources. I’m particularly enjoying threads by Dr. Natalie Dean (@nataliexdean), Dr. Caitlin Rivers (@cmyeaton), and Dr. Zeynep Tufekci (@zeyenp).
Dr. Yammine and infectious disease researcher Laurel Bristow are doing a lot of science communication around the virus on their Instagram accounts. Check their saved stories! They’re doing thorough research to find the evidence behind their explanations, and are also explaining newly emerging research from pre-prints.
Biology professor Dr. Erin Bromage went viral this month with a post about knowing the risks and avoiding them. He has been presenting solid facts for a general audience on his blog.
The models of COVID-19 mortality are not perfect. They come with uncertainties and predicted ranges that aren’t always reported or explained. They use parameters like case fatality rate, percent of contacts decreased by social distancing, and effective reproductive number which are different across populations and time. As is expected in science, the models are constantly being revised as new estimates for these parameters are available. An ensemble modeling approach, often used for forecasting even outside of disease outbreaks, may be more accurate. As National Public Radio (NPR) reports: “‘Individual models are being changed every week. They’re sensitive to the last observed data in different ways,’ says Reich. But with an ensemble ‘there’s a certain consistency and robustness. You’re not quite, sort of flapping in the wind.’”
Data Scientist Youyang Gu has a COVID-19 model that seems to be even outperforming the COVIDhub Ensemble model. From what I understand, it uses the classic epidemiology SEIR framework with machine learning to estimate the best parameters that go into the model (e.g. what is the reproductive number, Rt, at this time and place). You can see the historical performance for this model and other best-performing US models as compared to the CDC mortalities. I say all this to say, I’ve been intrigued comparing Gu’s models with reopening and without reopening. Please see this Twitter thread for some caveats of the model. Please note that it was recently reported (here and here) that the CDC and several states have been conflating the viral and antibody tests for COVID-19. They’re in the process of disaggregating the counts from the two tests, but this does mean some of the model’s input data is unreliable and unfortunately our estimates are only as good as the data that goes into them.
Imperial College London released a report on May 21, 2020 reporting new state-level tracking of COVID-19. Across the states they estimate the percent of total population likely to have been infected thus far. This ranges from 0.1% in Hawaii (95% confidence interval indicates the truth is likely in the range of 0.0-0.3%) to 16.6% in New York (with 95% confidence interval of 12.8%-21.6%) For several regions they show the reproductive number with respect to interventions such as business closures. In the report’s summary they state: “We predict that deaths over the next two-month period could exceed current cumulative deaths by greater than two-fold, if the relationship between mobility and transmission remains unchanged. Our results suggest that factors modulating transmission such as rapid testing, contact tracing and behavioural precautions are crucial to offset the rise of transmission associated with loosening of social distancing.”
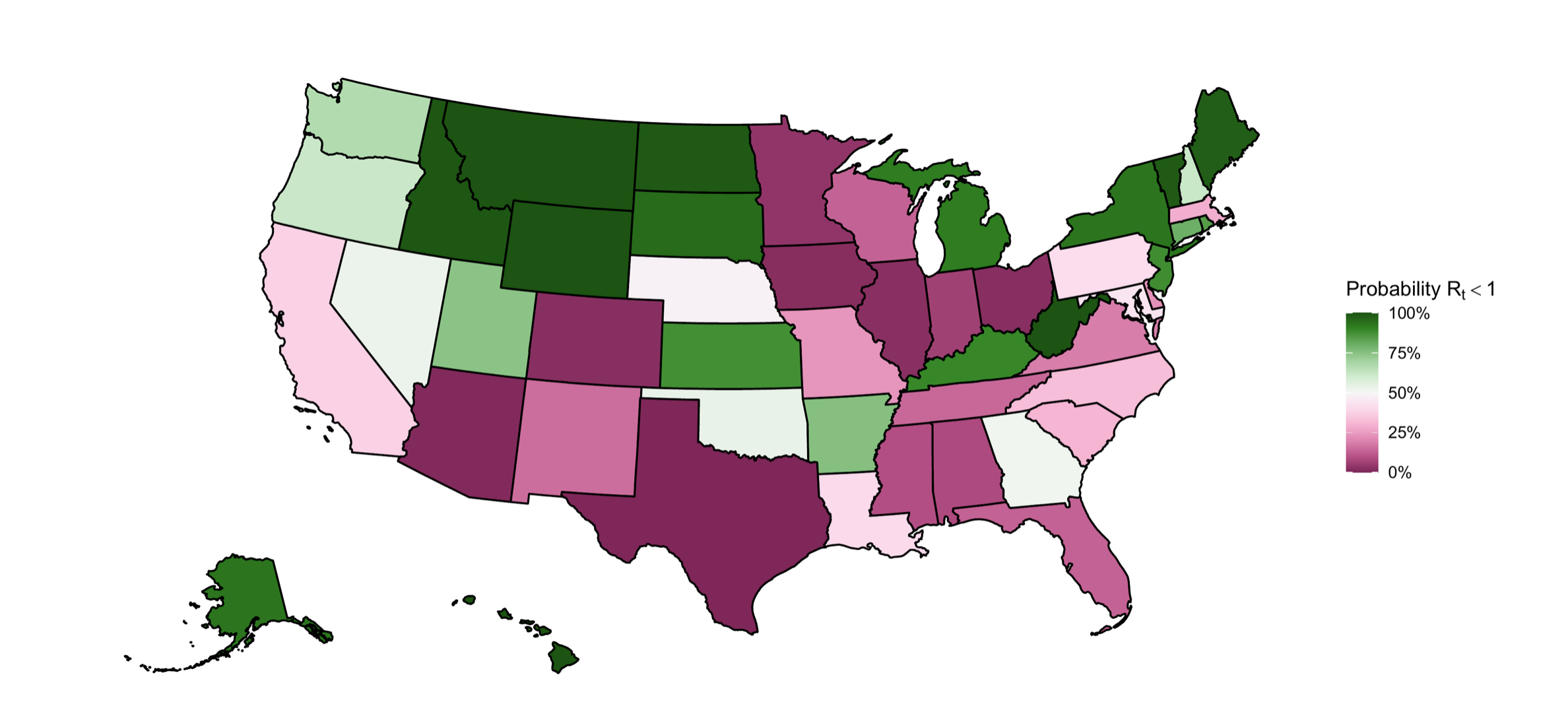
From the latest Imperial College London models, the probability that the reproductive number is <1 (representing epidemic control) for each state as of May 9, 2020. We want to be in the green.
Ultimately, the models are not perfect but they allow us to keep a pulse on potential outcomes given the level of non pharmaceutical interventions (NPI, e.g. social distancing) that we are following. Because of the longer time course for symptoms requiring hospitalizations, we may use models to put the brakes on ourselves before the car starts really rolling down the hill again.
(With regard to the introductory paragraph, I want to acknowledge the loss of life and quality of life to many non-Americans in these conflicts. By using this analogy, I in no way intend to minimize the pain the U.S. military has caused abroad, or even domestically. The ethics of war are important to consider but are not in the scope of this piece. I would also like to acknowledge the history of Memorial Day as it relates to the African American community in Charleston, SC honoring Union soldiers who died in the Civil War.)
]]>In my previous pandemic-related posts I’ve repeatedly encouraged readers to not believe everything you read on the internet, including my own editorializations and explanations. I do my best to highlight resources of interest and give explanations of scientific concepts (like R0 for viral transmission) or quirks of the scientific enterprise (pre-prints on biorxiv versus peer-reviewed journals). Because my training lies in genetics and statistics, I’ve tried to avoid topics that are incredibly outside my wheelhouse, and I do the requisite reading when explaining topics I haven’t been formally taught. I care most about pointing people to resources where they can see the data for themselves, but I know it may be challenging for those without a background in these fields to interpret the scientific data … it’s still difficult for me after 7 years of postbaccalaureate scientific training! So my other goal is to give non-experts tools to gauge the veracity of sources: is this peer-reviewed?, what is the scientific consensus on these findings?, are methods clearly explained?, is this an established source?, who is funding this?
Another science communicator, Dr. Samantha Yammine, provides advice for vetting sources at the end of a video explaining some inaccuracies in the Bakersfield doctors’ press conference: “At the end of the day don’t believe something someone says just because they have fancy letters at the end of their name or they’re in scrubs. If they’re pushing credentials on you and being overly assertive, in my book, that’s a red flag. Next time you see someone like that, especially if it’s someone, I don’t care who, going against what so many public health experts are saying, please reconsider spending your social currency on social media sharing it. And if you end up deciding you do want so share it, before you do that, try looking up if the opposite thing is true. Don’t look for what individuals are saying, try to get a sense of what consensus is, what majority of people are saying. While it is sometimes true that an individual is correct against all of the majority, it’s pretty rare, and if their evidence is spotty they’re probably not the exception.” If you’d like to learn more, North Carolina State University Libraries have a video about evaluating source credibility. I found two imperfect tools to gauge website credibility and bias–NewsGuard and Media Bias/Fact Check. It turns out, they are used by the University of Michigan School of Information Center for Social Media Responsibility to calculate an ‘Iffy Quotient’, or the percent or URLs with iffy credibility, shared on Facebook and Twitter at a given time.
This brings me to the credibility of a video which was circulating social media last week called “Plandemic.” It caused a stir with claims about aspects of the current pandemic and alleged controversies regarding HIV/AIDS and Ebola. I will not be linking to the video so as not to drive traffic to what many scientists and doctors believe to be a dangerous piece of misinformation from an uncredible source, although a full transcript is on Medium. Lots of people have done the necessary work to provide evidence refuting the video’s claims. To be clear, I do not think scientists and medical professionals are infallible, I acknowledge that unethical behavior occurs, and I am not so naive as to believe those in power are immune to ulterior motives. But extraordinary claims require … evidence. Thus far, there is very little evidence supporting the video’s conspiratorial claims. Below is a synopsis of places to find information about “Plandemic” and I summarize some lessons learned for my scientist colleagues.
Several science journalists and others have attempted to verify the claims with evidence, publications, etc:
A few Facebook posts that have gained traction that attempt to provide alternative perspectives:
There was also a fact check by Dr. Mike with a YouTube video if you’d prefer video format.
For scientists reading, I posit this is a unique time for us to take a more direct approach at
1) educating the public about our tax-payer funded research (COVID-19 related or otherwise)
2) engendering public trust by explaining who we are and our motivations and
3) empathetically correcting misinformation with scientific evidence when we are able.
Tara Haelle covered a lot of this in her piece for Forbes. I’ve reflected on some lessons for the scientific community based on the comments from my own Facebook post that garnered quite a lot of debate.
Some believers of “Plandemic” are those who engage in conspiratorial thinking. There is a rich body of peer-reviewed research on conspiracy theories. With a quick search I found this, and I’ve seen this recommended to better understand where some people are coming from. Showing empathy, affirming critical thinking, and avoiding ridicule are important here. More specific to the time at hand, this peer-reviewed work examined why people believe COVID-19 conspiracy theories. They found “beliefs in two popular variants of COVID-19 conspiracy theory are the joint product of the psychological predispositions 1) to reject information coming from experts and other authority figures and 2) to view major events as the product of conspiracies, as well as partisan and ideological motivations.”
Some people have internalized misinformation without recognizing it as such, and the “Plandemic” video further confirms what they’ve heard through confirmation bias. In 2018, a study showed falsehoods on Twitter spread faster, deeper, and broader than the truth. A recent article in The Atlantic by misinformation expert Renee DiResta, highlighted the need to combat misinformation: “If institutions and authority figures don’t adapt to the content and conversation dynamics of the day, other things will fill the void. The time for institutions and authorities to begin communicating transparently is before wild speculation goes viral”. Another piece in The Atlantic by Yale lecturer, Liz Neely, walks us through ways to help others be better informed about the pandemic. Start with people who know and trust you, pick your battles, affirm shared values, start the conversation broad without jumping to correct the misinformation, and be honest and transparent.
Some believers of “Plandemic” are not sure who to trust and may not have the prior knowledge to come to their own conclusions. To assist these individuals, here is a list of topics I believe we should try to clarify to non-experts when given the opportunity. Topics related to COVID-19 misinformation specifically are italicized. A lot of them deal with the systems and checks and balances that we know exist in settings across academic and government biomedical research, but are quite opaque to the rest of the world: the peer-review process, pre-prints, retractions, grant funding, study sections, academic hierarchies (phd candidate, graduate student research assistant, postdoc, assistant professor, tenure), salary, conflict of interest disclosures, technology transfer, personal motivations for pursuing science, salary, universities versus private research institutes versus governmental research organizations, the scientific method, the iterative process of science, necessary vs sufficient, correlation vs causation, institutional review boards, how ethics violations are handled, the organizational structure of NIH and NSF, replication studies, patents for biomedical research especially vaccines, the Bayh-Dole Act, clinical trials, pharmaceutical pricing, the role of pharmaceutical companies in research, the reason for pandemic preparedness exercises like this, the uncertainty around models including 95% confidence intervals
I observed common beliefs that provide some additional perspective to consider as we communicate moving forward:
Any association with mainstream media (although what is considered mainstream is heterogeneous amongst individuals) automatically discredits information that lies therein, even when it was formerly a trusted source. When presenting evidence, we may have to select new sources that a given individual trusts. For example,
A: I’ll believe Plandemic when I see it on 60 Minutes
B: 60 Minutes is produced by CNN and CNN lies all the time (Fact check: 60 Minutes is produced by CBS News)
A: Really! I didn’t realize :(
“I believed this until I realized you worked for the government.” That the government is not trusted will come as no surprise, but you can read about 2019 Pew Research Center results about trust and distrust in American government.
“I don’t trust scientists.” Pew Research shows trust in scientists in on the upswing in America, but the non-random sample of the Facebook post comments represents many that don’t trust scientists. Perhaps proactively communicating our science and engendering public trust would bolster trust in science in times of crisis. Some also suggest that the general public needs to have their expectations tempered for what the experts can and can’t know. “We need to value scientists and listen to experts, but part of listening means understanding that right now, what they’re saying is that they do not have all the answers.” Maybe that starts with scientists making our limits of expertise more clear by normalizing the phrase “I don’t know.”
“The truth is somewhere in the middle.” I would posit that when 99 experts say position A and one expert says position B, the onus is on the one expert to provide unassailable evidence to move the needle anywhere towards middle ground. However, I saw this comment frequently, with many claiming neutrality with regard to claims in ‘Plandemic’. The existence of a middle ground is impossible when one position is a verifiable piece of misinformation. Although simplistic, if 99% of experts say the sky is blue and 1% say the sky is red, it doesn’t mean the sky is purple. Being aware of this common attitude could be informative in future conversations.
It was obvious many people had genuine questions. Here are the few I had the time to tackle in case the answers are helpful for you in your discussions with others. If one had unlimited time, I’m sure they could be better researched or supported. For most facts I only provide one citation, but I believe finding credible sources that converge on similar findings is key.
Q: Why are we shutting down for a disease with 99.6% survival rate?
A: In terms of the survival rate for COVID-19, epidemiologists often talk about the inverse of this—-the infection fatality rate (IFR) which is the number of deaths of all infected cases, not just the ones we have found by testing or hospitalization. You can read more about IFR and case fatality ratio (CFR) as they relate to COVID-19 here. In summary, IFR is estimated for a given population and can increase due to overwhelmed hospitals, poor underlying health, older populations, etc. These rates can also decrease as medical professionals become more skilled at treating the disease. I say all this to indicate there is uncertainty involved in estimating what proportion of people die from COVID-19. Right now we aren’t testing enough people to know our infection fatality rate (IFR), because infections are happening that aren’t recorded as cases. As we perform seroprevalence surveys to test for antibodies, we can understand how many have been infected and therefore estimate IFR. Early work does point to a fairly low IFR in some populations but there are limitations to these studies and we need more data! But the early IFR estimates for COVID-19 are greater than the 0.004% IFR for the flu for example (here is a Twitter thread with a publication). If the IFR is 0.4% and we multiply this by the millions in the U.S. who would be infected (let’s say 50%, which is a conservative estimate of herd immunity, of our 328 million population) we would have 656,000 deaths over some period of time, maybe a year. The larger concern is that COVID-19 can spread exponentially in a population with no vaccine and no immunity from previous infections. This can overwhelm health systems resulting in more deaths and a larger IFR. Many of the states’ stay at home orders reduced transmission (as seen by decreased hospitalizations in NY and MI, for example) to provide time to prepare hospitals and increase capacity for contact tracing which will be very important!
Q: Won’t washing my hands so much remove the good bacteria on my hands and therefore weaken my immune system?
A: It sounds like you’re interested in the microbiome, I am too! Our skin microbiome has transient flora which we get from touching objects and resident flora which is what would be important for our immune systems. Soap, warm water, and friction can physically break down the virus, and you don’t need to use anti-bacterial soap to remove the SARS-CoV-2 virus from our hands. The normal bacteria that colonize our skin, what we call the skin microbiome, will remain intact through frequent hand washing because they’re in the superficial layers of our skin and can also regrow if some of it is removed from hand washing. You can read more here.
Q: What about carbon dioxide poisoning from wearing masks?
A: Here is a fact check by Reuters. The amount of CO2 the average person would breathe in from a cloth mask for time spent in public is not dangerous. I can see why many people find them hot and stuffy, I do too, but it’s important to me to protect others around me in the event I’m sick and don’t realize it. Even more restrictive face masks like N95 respirators (which the public is not being asked to wear) are used frequently in professions like construction and medicine. I searched PubMed for peer-reviewed research and did see several small studies had measured the elevated carbon dioxide in the “dead-space” of N95 filtering facepiece respirators (e.g here), but I saw no evidence that this is so dangerous as to not use them to prevent infection.
Q: How do you explain this research if chloroquine isn’t an effective treatment?
A: There are a few reasons why the findings in this paper can’t be directly applied to the current pandemic. It is about the original SARS virus and not the novel coronavirus, SARS-CoV-2, which causes COVID-19. This paper showed therapeutic benefit in primate cells (what we call in vitro), but didn’t demonstrate effect on a living human (in vivo) which can sometimes have different outcomes than studies in cell lines. The drug in this study is called chloroquine, it’s closely related to hydroxychloroquine. Both chloroquine and hydroxychloroquine are being used in randomized controlled trials, the gold standard of medicine to prove drug efficacy. A pre-print (not yet peer-reviewed) showed the drug did not reduce the risk of mechanic ventilation and there was increased death in those treated with hydroxyochlorquine. A peer reviewed observational study showed the drug was not associated with increased or decreases intubation or death. Study results are still coming out, but the early signs show this drug could do more harm than good by causing heart rhythm abnormalities. I know some early studies in small sample sizes and anecdotal evidence looked like hydroxycholoroquine was a promising treatment, but science is iterative and we update standard of care when we learn more.
Q: The Pirbright Institute has a US patent on the coronavirus and Vanderbilt owns a large number as well. See here.
A: Coronaviruses are a broad class of viruses with some causing the common cold and others like SARS-CoV-1 causing the 2003 SARS epidemic. The novel coronavirus, SARS-CoV-2, which causes COVID-19 is different from this patent. The link you provide regarding the Pirbright patent says: “DISCLAIMER: Coronavirus is a broad name for a family of viruses. This patent is NOT for the new COVID-19 virus and The Pirbright Institute does not currently work with human coronaviruses. If you share this patent online, be aware you are in fact sharing a separate patent for avian infectious bronchitis virus and porcine delta-coronavirus. This is not a patent for the new COVID-19 virus.” The world of patents in medicine is definitely a complicated one, so I understand how this might be confusing.
Q: Didn’t Dr. Fauci say they were using previous research and the existing coronavirus vaccines to jump start the process for finding a vaccine for the novel coronavirus? His comments suggested they were much closer to a new vaccine because of the previous work they had done. And this wasn’t originally a human coronavirus, was it?
A: Previous research on coronaviruses has been really helpful in the effort to quickly create a safe and effective vaccine to help curb the spread of COVID-19 across the world. That being said, I believe in vaccine safety and clinical trials are underway to ensure even the vaccines produced are safe. Because the previous SARS pandemic in 2003 and MERS outbreak in 2012 were both from types of coronaviruses, many scientists have been aware of the continued risk of coronaviruses jumping from animals to humans. This is called a spillover event, and this page has a bit more information. You can read a comparison to SARS-CoV which caused SARS and SARS-CoV-2 which causes COVID-19. Because of the inevitability of another coronavirus outbreak, scientists have been working on vaccines that can target these types of viruses. The NIAID has a nice video from January explaining their vaccine research (many organizations across the world are working on vaccines that have different mechanisms). This article also touches on the fact that because of their work with MERS, scientists know how to optimize vaccines that will target the spike protein seen on the coronavirus that causes MERS and the coronavirus that causes COVID-19. I hope this also answers your question regarding if this was originally a human coronavirus. The exact origins of the virus have not been confirmed, but scientists are confident that is has natural origins with a spillover event from an animal like previous coronaviruses. You can read more here, here, and here.
Q: A secondary interview with one of the Bakersfield doctors seems to clarify their original points, what do you think?
A: Here is the joint statement that was issued by two professional organizations for emergency medicine. It has an additional information section which describes how difficult it is to compare flu versus COVID-19. I disagree that there isn’t data supporting social distancing and isolation. Peer reviewed work in a well respected journal, JAMA, showed that non pharmaceutical interventions (NPI, the technical term for mitigation strategies like social distancing) reduced the Rt (average transmissions one infected person makes) substantially in China (Figure 4). A pre-print looking at 20 countries showed the reduction in number of new cases from a variety of mitigation techniques like quarantine. We even know social distancing worked in the 1918 pandemic. There are many popular science articles about this, but I found a peer-reviewed article from before COVID-19.
He states there are 14 patients hospitalized in his county for flu, 3 on ventilators. I would need to know how many were hospitalized with COVID-19 on the same day to put those numbers in context with the point he is trying to make. I tried to make a similar comparison from their public health website. The county had 9 deaths for flu in 2018-2019 season and has already had 15 resident (10 if you count non-resident) deaths in the first few months of the pandemic. We know the flu has demonstrated seasonality, but we don’t yet know if COVID-19 will have seasonality meaning it could continue to move through an immunologically naive population (without a vaccine like we have for flu) all summer making for a much longer “season”. Here is a pre-print discussing projections for the summer. But because the flu and COVID-19 are still so different (length of treatment longer with COVID-19, difference in way of counting deaths, constellation of complications presenting with COVID-19) I hesitate to put much weight in these comparisons.
The ultimate goal is herd immunity, but no one is advocating for shelter in place until then. As he mentions, there is collateral damage of shutting down the economy—-the public health ramifications from economic downturns are real and weigh heavily in all of our minds. From my reading, I believe most epidemiologists would say the strategy for a country like the U.S. which had such widespread community transmission is to reduce Rt with suppression strategies (e.g. shelter in place) before carefully re-opening and beginning test, trace, isolate. This prevents health care systems from being overwhelmed, provides time for PPE manufacturing and therapeutic development, and builds confidence in consumers for participating in the economy, etc. Then we reach herd immunity by combination of the virus moving more slowly through the population and a vaccination program when one is available. If we reach herd immunity by letting the virus run through the population, by assuming Rt of 3 and a fairly low infection fatality rate (IFR) of 0.2%, that would mean ~350,000 deaths in the U.S.(Figure 2C). Scientists are in the process of figuring out a more accurate IFR through seroprevalence studies, but I’ve seen early estimates around this value. I acknowledge the model’s assumptions are not perfect and are being revised and replicated by different groups. You can see in that figure that Sweden has a much lower predicted mortality than the US. I think this opinion piece describes my position on Sweden pretty well—-there’s a lot we still don’t know!
Q: Didn’t Dr. Judy Mikovits worked for Dr. Fauci because he is at the NIH and so was she? A: I cannot find Dr. Mikovits’ CV online, but according to her Wikipedia page and the affiliations I see on her published papers, she never worked at National Institute of Allergy and Infectious Disease (NIAID) where Dr. Tony Fauci is the director. As I stated in my original post, NIAID is one of 27 institutes and centers of the National Institutes of Health (NIH). It appears the bulk of Dr. Mikovits’ work was at a different institute, National Cancer Institute (NCI), and a private research institute, Whittemore Peterson Institute. Therefore she would have never been in a direct reporting line of Dr. Fauci. I also provided as a caveat, it’s possible that she received extramural grants from NIAID at some point in her career. Regardless, in the world of science you only “work for” someone if they are the principal investigator (PI) of your laboratory or you’re a PI and they are a departmental/branch chair. If you work for someone you’d likely be on papers with them as co-authors, and a search of PubMed shows Dr. Fauci and Dr. Mikovits are not co-authors on any publications that I can find.
]]>Let’s begin with a statistics primer. When statisticians try to assess statistical differences between groups, we perform hypothesis testing. We determine a null hypothesis, which is a statement claiming no relationship between two measured phenomena (treatment and outcome) or between specified populations (the group receiving a drug and the group receiving placebo). We then consider an alternative hypothesis, which basically says there is, in fact, a difference between the two groups. We cannot prove the alternative hypothesis, but we can reject that the null hypothesis was likely to have produced the observed data. We then decide what false positive rate we are willing to live with. That means, are we willing to incorrectly reject our null hypothesis some percent of the time. We call this the alpha level, or significance level, and in standard practice it is 5%. Here is a video from Khan Academy if you want to learn more.
The output of many statistical methods is a p-value, or probability value, which is the probability of obtaining results at least as extreme as the observed results of a given experiment, assuming the null hypothesis is correct. A p-value of 0.05 means if we completed 100 identical experiments, we could see results this extreme or more extreme in 5 of the experiments simply due to chance. The American Statistical Association has an informative editorial on p-values.
In practice, we use the significance threshold to dichotomize our findings as significant (p-value < 0.05) or not significant (p-value ≥ 0.05). But the quantitative nature of the p-value really gives us evidence that exists on a spectrum of 0 to 1. For example, observations with a p-value of 0.04 and 0.00000004 are treated the same, as significant findings. But a p-value of 0.04 and 0.06, while much closer in magnitude, are considered significant and non-significant, respectively. There is a lot of debate within the scientific community about p-values, determining significance, etc. You can read more here, here, and here. It’s a big ol’ can of worms that you should be aware of, but we don’t need to open to understand the findings of the remdisivir trial.
The trial looked at two outcomes: recovery time and mortality (aka death). Those receiving the treatment had a median time to recovery of 11 days versus 15 days for those receiving the placebo. Recovery was defined as hospital discharge or a return to normal activity. A statistical test was done to compare the median recovery time between these two groups. The null hypothesis here is that there is no difference in the median recovery time between the treatment and control groups, and the alternate hypothesis is that there is a difference. If we set our alpha at the standard significance level of 0.05, then with the reported p-value being less than 0.001, we would reject our null hypothesis. We interpret this hypothesis testing to mean there is a difference between the treatment and control groups which is so great we would only expect to see it by random chance in less than 1 in 1000 experiments. We can feel pretty confident that the treatment is responsible for the 31% faster time to recovery observed in this sample. However, it is unclear to what extent this modest effect will change the course of the pandemic.
For mortality as an outcome, 8% of the treatment group died versus 11.6% of the placebo group. The p-value for comparison between groups is 0.059, so with the same significance level of 0.05, we would not be able to reject our null hypothesis. But this doesn’t mean we accept the null hypothesis that there isn’t a difference in mortality between the two groups. It just means we just haven’t amassed enough evidence to prove there is a difference within the false positive rate we decided would be acceptable (0.05). This could provide enough hope that there is a difference between groups to encourage further study, potentially in larger samples.
An independent data and safety monitoring board (DSMB) reviewed the data and shared the interim analysis with those running the study. The DSMB is a committee of experts responsible for reviewing clinical trial data to preserve study integrity. Because of this, we can be hopeful that no one with a vested interest in the pharmaceutical company’s fortunes or political incentives could sway the outcome of the clinical trial.
A formal report should be released in the coming weeks and we will know more about the study limitations. You can read Gilead’s statement too. The NY Times is reporting the FDA plans to announce as early as today the emergency use authorization for remdesivir. My personal take is this is obviously not the panacea we were all hoping for, and I hope the additional treatments in development or trials will prove more effective.
Here are additional news & views:
A retrospective analysis (scientific analysis happens after events occur) of 368 patients seen through the US Veterans Health Administration suggest hydroxycholoroquine is not helpful as a COVID-19 treatment and may even be associated with worse outcomes. In a recent pre-print researchers showed that patients treated with hydroxychloroquine were more likely to have died than the control group (hazard ratio 2.61 with 95% CI 1.10-6.17), but there was not a significant association between treatment and death/survival for those receiving hydroxychloroquine and azithromycin (a common antibiotic). Randomized controlled trials are ongoing and will provide clear guidance on use of this drug. A correspondence was recently published in Nature Medicine described incidence of heart abnormalities in patients treated with hydroxychloroquine and azithromycin. In 84 patients the baseline average QT-interval, a measurement used to assess the electrical signals in the heart, was prolonged from 435±24 ms to 463±32 ms. In 9 patients (11% of cohort) the prolongation was severe to the point of putting them at risk of sudden cardiac death. This is one of the risks of using this drug as a potential treatment.
Community transmission was occurring so early in the U.S. that a non-travel related COVID-19 death has been confirmed from February 6 in California. Read the press release from Santa Clara county and NY Times reporting. With this timestamp it’s clear that we were really shockingly behind at preventing this from spreading in the United States. This lines up with virologist Dr. Trevor Bedford’s work showing first U.S. introductions in January 2020 as explained here.
The CDC released characteristics of patients hospitalized with confirmed COVID-19 in the 4 week period ending March 28, 2020. In the Morbidity and Mortality Weekly Report they describe 89.3% to have one or more underlying conditions with the most common being hypertension (49.7%) followed by obesity (48.3%) which are also fairly common co-morbidities in the United States. “Among the 1,482 laboratory-confirmed COVID-19–associated hospitalizations reported through COVID-NET, six (0.4%) each were patients aged 0–4 years and 5–17 years, 366 (24.7%) were aged 18–49 years, 461 (31.1%) were aged 50–64 years, and 643 (43.4%) were aged ≥65 years.”
The NIH Director, Dr. Francis Collins, highlighted the challenge of tracking the virus’ spread on his blog. Traditional containment strategies are testing of symptomatic cases, contact tracing and quarantine. Due to the spread of disease before symptoms or even without symptoms, we need to expand the goals of testing to 1) help us identify asymptomatic people infected by SARS-CoV-2 to initiate quarantine so they cannot infect others 2) understand who has recovered from SARS-CoV-2 and may now possess immunity. The National Institute of Allergy and Infectious Disease (NIAID) released their strategic plan for COVID-19 research for the next four years. The main priorities are
1) Improve knowledge about the virus and the disease
2) Support development of diagnostics and assays (i.e. testing for the disease or antibodies)
3) Characterize and test therapeutics to treat the disease
4) Develop safe and effective vaccines against SARS-CoV-2
In addition, the NIH recently announced a public/private partnership to speed COVID-19 vaccine and treatment options. The Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) partnership will focus research and development efforts. The World Health Organization also announced worldwide collaborations to accelerate development of COVID-19 health technologies and ensure their equitable access across the globe.
Facebook and Carnegie Mellon have collaborated on a survey and have released preliminary data as a COVID-19 Symptom map.
Data viz of COVID-19 spread in the U.S. since January 2020 by University of Michigan PhD Candidate Marlena Duda
Belgian and Dutch engineers released a white paper concerning optimal distancing between individuals during movement (walking, running, biking). While 1.5 meters or 6 feet is a good rule of thumb for people standing apart, these engineers’ simulations show a greater distance should be maintained during activity. The risk of contamination by large microdroplets is greatest when walking or running directly behind another person and 4-5 meters (13-16 feet) should be maintained to avoid moving through this cloud of particles. This work hasn’t been released on a typical pre-print server so I’m unable to evaluate the findings based on the reactions of other experts. Based on this work, I think it’s good to consider maintaining maximum physical distance and keeping 6 feet as our “worst case scenario” of proximity.
A report published in the journal Science with research by Harvard epidemiologists made headlines yesterday for its conclusion that prolonged or social distancing may be needed into 2022. They modeled transmission using estimates of seasonality (e.g. viral disease transmission tends to decrease overall in the summer), immunity (duration of immunity from antibodies in people who have already fought the infection), and cross-immunity (the possibility that exposure to existing mild to moderate coronavirus strains may provide protection against SARS-CoV-2). They looked at several different scenarios, for example the one time social distancing we are experiencing now, of various durations, both with and without virus seasonality. They also considered intermittent social distancing in a world with our current critical care capacity in the nation’s hospitals and with extended capacity. There are plenty of limitations thoughtfully outlined in the discussion, for example, it is unknown how long an infected person will maintain immunity (that’s why serology testing to understand this is so important). These scenarios will change in the presence of vaccines or other interventions such as aggressive contact tracing and quarantine. The authors conclude the total incidence of the virus through 2025 will depend on the duration of immunity and the cross-immunity with other coronaviruses. A key paragraph emphasizes why this research is important:
“Intermittent distancing may be required into 2022 unless critical care capacity is increased substantially or a treatment or vaccine becomes available. The authors are aware that prolonged distancing, even if intermittent, is likely to have profoundly negative economic, social, and educational consequences. Our goal in modeling such policies is not to endorse them but to identify likely trajectories of the epidemic under alternative approaches, identify complementary interventions such as expanding ICU capacity and identifying treatments to reduce ICU demand, and to spur innovative ideas to expand the list of options to bring the pandemic under long-term control”
An antiviral that can be taken in pill form, EIDD-2801, is showing some promise. NPR covered this and the research was published in Science Translational Medicine. β-D-N4-hydroxycytidine (aka NHC, EIDD-1931) is an antiviral known to work against RNA viruses like influenza and Ebola and it was “potently antiviral” (i.e. it worked) against SARS-CoV-2 and other related coronaviruses in infected cell lines and primary human airway cell cultures (what we would call in vitro). A prodrug, which means it is converted to the active drug inside the body, of EIDD-1931 called EIDD-2801 was already optimized for use as a medicine for humans. They tested EIDD-2801 in mice who were infected with a mouse-adapted version of SARS-CoV and found it was “potently antiviral”, but clinical benefit was best when administered ~24 hours after infection. They concluded that more research was needed, but any research on coronavirus treatments is relevant for this pandemic and future ones. While we should temper our expectations for EIDD-2801 becoming an immediately useful therapeutic, all new scientific evidence in this space is inching us forward.
An important addition to this final point from April 23, 2020. NPR is reporting that virus researchers who are experts in this kind of lab work say “there is virtually no chance that the new coronavirus was released as a result of a laboratory accident in China or anywhere else.” I weight this evidence more strongly than the previously reported tenuous evidence about laboratory problems from China.
]]>The CDC has issued guidelines recommending all Americans to wear homemade masks when out in public. This does not mean you should go buy hospital-grade personal protective equipment (PPE). Please save that for the health care workers! But what led to this new recommendation?
I watched an event tonight with NIH Director Dr. Francis Collins hosted by Biologos, and he reiterated that the virus is primarily transmitted via droplets from sneezing and coughing. However, he mentioned unpublished work by an NIH investigator that used laser technology to show that speaking was emitting droplets that could contain viral particles. This is the main argument for why we should be wearing masks out in public now. He reiterated that we’re being asked to wear masks not to protect ourselves, but to protect someone else on the chance that we are infected and don’t know it. Staying 6 feet apart remains a critical part of reducing transmission.
On the other hand, health care workers need masks to protect themselves from infected patients, and that’s where an N95 respirator is key. This naming convention comes from the National Institute for Occupational Safety and Health (NIOSH) air filtration ratings with N meaning “Not resistant to oil” and 95 meaning the respirator has a 95% efficiency for filtering particles of 0.3 micrometers, and a greater than 95% efficiency for particles less than and greater than 0.3 micrometers. Respiratory droplets are 5 to 10 micrometers in size. A study from Korea found the virus to be 0.07-0.09 micrometers in size. Smaller droplets called bioaersols can be produced when we talk and breathe, and these can travel further and stay in the air long. The virus can also be aerosolized during medical procedures like intubation which one reason our health care workers need proper PPE.
The prestigious National Academies of Sciences, Engineering, and Medicine has a Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats. Their communication to the Executive Office of the President laid out the current scientific evidence for viral transmission as of April 1, 2020. Some of the evidence is in pre-prints, these are publications by bonafide scientists that have not be subjected to the usual peer review but allow rapid dissemination of findings. Among the research presented was evidence from Nebraska which detected viral RNA from air collectors greater than 6 feet away from COVID-19 patients. Just because viral RNA is present doesn’t mean the virus would remain infectious, but it does mean particles are likely travelling as bioaerosols. Samples taken from hospitals in Wuhan suggested the virus may be resuspended as an aerosol by PPE removal or cleaning procedures in hospitals, but encouragingly found undetectable or very low concenrations of SARS-CoV-2 aerosols in public locations. The two key sentences of the letter are “Currently available research supports the possibility that SARS-CoV-2 could be spread via bioaerosols generated directly by patients’ exhalation.” and “However, for no respiratory virus is the exact proportion of infections due to air droplet, aerosol, or fomite transmission fully established, and many individual factors and situations may contribute to the importance of each route of transmission.” The scientific evidence laid out in the letter is thought to be the driving force behind the CDC recommendation. Here is a nice piece by NPR on the droplet transmission of the virus.
Transmission by pre-symptomatic cases is another motivator for wearing masks, so you can protect others before you know you’re infectious. A study out of China showed SARS-COV-2 is more efficiently transmitted than SARS-CoV, the virus responsible for the 2003 SARS epidemic, largely through active viral shedding at a time when symptoms are still mild and indicative of an upper respiratory infection (in the throat as opposed to lung).
Another piece of the puzzle is the unknown prevalence of asymptomatic cases. As early as January there were case reports emerging from China of asymptomatic carrier transmission. The journal Nature summarized research in this space as of March 20, 2020. A NEJM correspondence regarding a small sample from China showed an asymptomatic patient had a similar viral load (e.g. amount of virus present) to the symptomatic patients in a nasal and throat swab.
As I highlighted on the March 16, 2020 Update, testing on the Diamond Princess Cruise ship showed 50.5% (320 of 634) of positive cases to be asymptomatic. Statistical modeling allowed researchers to estimate how many were likely to develop symptoms after the time of observation. They estimated that 17.9% (95% confidence interval of 15.5-20.2%) of positive cases were truly asymptomatic.
Widespread testing in Iceland by deCODE genetics was recently published in a non-peer-reviewed pre-print. Since testing capacity is limited in most countries, we generally only know about COVID-19 test results in high-risk populations (e.g. very sick patients in the hospital, health care workers). In Iceland they screened a mostly random sample of the population (N=5,502) and found 0.9% to be positive for COVID-19. 33 of the 50 (66%) with a positive test from the population screening had symptoms meaning 34% were asymptomatic or pre-symptomatic. On the other hand, the targeted screening yielded 10.1% positive of 1,928 (86.4% with symptoms) from the time frame February 1 to March 15 and yielded 13.4% positive of 2,623 (92.6% with symptoms) from the time frame March 16 to March 22.
A French publication, RFI, interviewed an Italian virologist who tested the entire population (N=3,300) of a small town, Vò, in Northern Italy. They found 3% of the population to be positive and the majority did not have symptoms. Unfortunately I haven’t seen data or additional details for this study.
Because the estimate of asymptomatic case prevalence ranges quite a bit, you might be tempted to throw up your hands and believe none of it. In statistics we note limitations to population-specific estimates by reminding readers that each population has its own quirks or the ascertainment of cases in different populations may vary. Despite the estimate’s uncertainty, the findings can still point us to a conclusion that asymptomatic and pre-symptomatic cases can spread the virus. Hence the importance of wearing masks in public! Please read important information from the World Health Organization (WHO) about how to safely put on, wear, and remove a mask is here.
A vaccine was tested in mice using microneedle arrays instead of the normal subcutaneous (e.g. under the skin) needle injection. The immune response was found to be stronger with the skin-targeted delivery than the normal injection. The immune system’s response is measured by a technique called ELISA (enzyme-linked immunosorbent assay) which can quantify the amount of antibody present in the blood. They found the mice developed antibody responses specific to SARS-CoV-2 within 2 weeks of immunization. This group was poised to work on the vaccine due to previous work developing a microneedle array vaccine for MERS. In fact, since the viruses are so similar, their longterm evidence of the vaccine’s ability to generate long lasting (> 1 year) antibodies is encouraging that the same will be true for the SARS version. They are hoping to start a phase 1 human clinical trial soon. You can read the scientific paper and the press release from University of Pittsburgh. There are teams all over the world working on potential vaccines. This is good news because we have more chances for one to work, and if multiple work then we can scale up society-wide immunization sooner. The first U.S. phase 1 clinical trial began in mid March for a vaccine made by National Institute of Allergy and Infectious Disease (NIAID) scientists and Moderna. A commentary in The Lancet elaborates on the three imperatives for vaccine development: speed, manufacture and deployment at scale, and global access.
We hear about the respiratory problems of COVID-19 patients, but doctors are also finding cardiovasacular issues. In an investigation published in JAMA Cardiology, scientists in Wuhan retrospectively (e.g. observed after the outbreak) analyzed 187 patients from January 23 to February 23. 27.8% exhibited myocardial injury, which means damage to the heart muscle. This myocardial injury is associated with fatal outcome, as well as cardiac dysfunction and arrhythmias. However, patients with underlying heart disease who do not experience myocardial injury had a relatively favorable outcome. In order of largest to smallest percentage of in-hospital fatalities 1) heart disease + myocardial injury 2) myocardial injury only 3) heart disease without myocardial injury 4) neither heart diseae or myocardial injury (please see Figure 2). There’s a lot of debate regarding the mechanism of action for this damage. Perhaps the virus is infecting the heart and causing damage or maybe the body’s immune system is causing damage. Kaiser Health News, which is an editorially independent program of Kaiser Family Foundation (not associated with health insurer Kaiser Permanente) published an in-depth piece on COVID-19 associated heart damage.
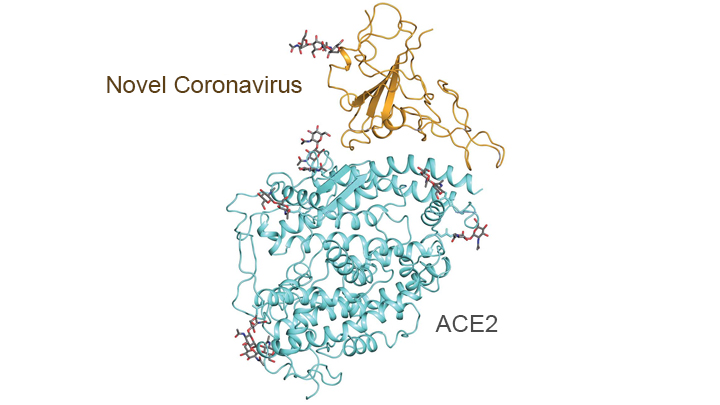
A recent study used a method called cryo-electron microscopy to visualize the interaction of human protein and the SARS-CoV-2 virus. Knowing the structure will be helpful for developing therapeutics. The virus’ spike protein binds to angiotensin-coverting enzyme 2 (ACE2) which is expressed in lung, hence the predominantly respiratory nature of the illness. Because angiotensin-coverting enzyme (ACE) inhibitors are used to treat high blood pressure and heart failure, clinicians wondered how this drug would interact with viral infection. Another study determined that ACE inhibitors (and the broader class of renin-angiotensin-aldosterone system [RAAS] inhibitors) can be continued in COVID-19 patients, although they caution more study is needed in this area. This was all summarized in a blog post by NIH Director Dr. Francis Collins.
|
Molecular map showing interaction between the spike protein (gold) of the novel coronavirus and the peptidase domain (blue) of human angiotensin-converting enzyme 2 (ACE2). Credit: Adapted from Yan R., Science, 2020 for the NIH Director’s blog.
A specific model for North Carolina was created by independent NC epidemiologists and data scientists.
A specific model for Michigan was created by university of Michigan epidemiologists.
The University of Washington’s IHME updated their models on April 5 and they describe these changes transparently and in-depth. State-level hospital use and the impact of social distancing provided a lot more information for parameter estimates. Overall the forecasts are more favorable but the estimates have a larger uncertainty.
Here is a beautiful explanation by a respected science writer, Carl Zimmer. He explains how each of the segments of the viral RNA create proteins that perform specific tasks. The structure of the virus is important to finding drug targets as Dr. Francis Collins highlights in his NIH blog, mentioned above.
Yale created an illustrated scientific summary of how the virus causes COVID-19 symptoms and how it is spread.
A visualization comparing daily COVID-19 deaths to other top causes of death in the U.S.
I am also seeing decades of unaddressed health disparities multiplying the pandemic’s effects in cities I love like Detroit, Michigan. Health disparities remain a complex issue with a body of scientific literature but few robust solutions. Unfortunately, the same co-morbidities and chronic conditions that increase COVID-19 complications and fatalities (heart disease, diabetes, and lung disease) are the same ailments that concentrate in communities that have been historically disenfranchised and face systematic racism, food insecurity, under-insurance, etc. How do you follow CDC recommendations for hand washing when your water is cut off? You can educate yourself on health disparities here. You can read about health disparities in the face of COVID-19 here and here.
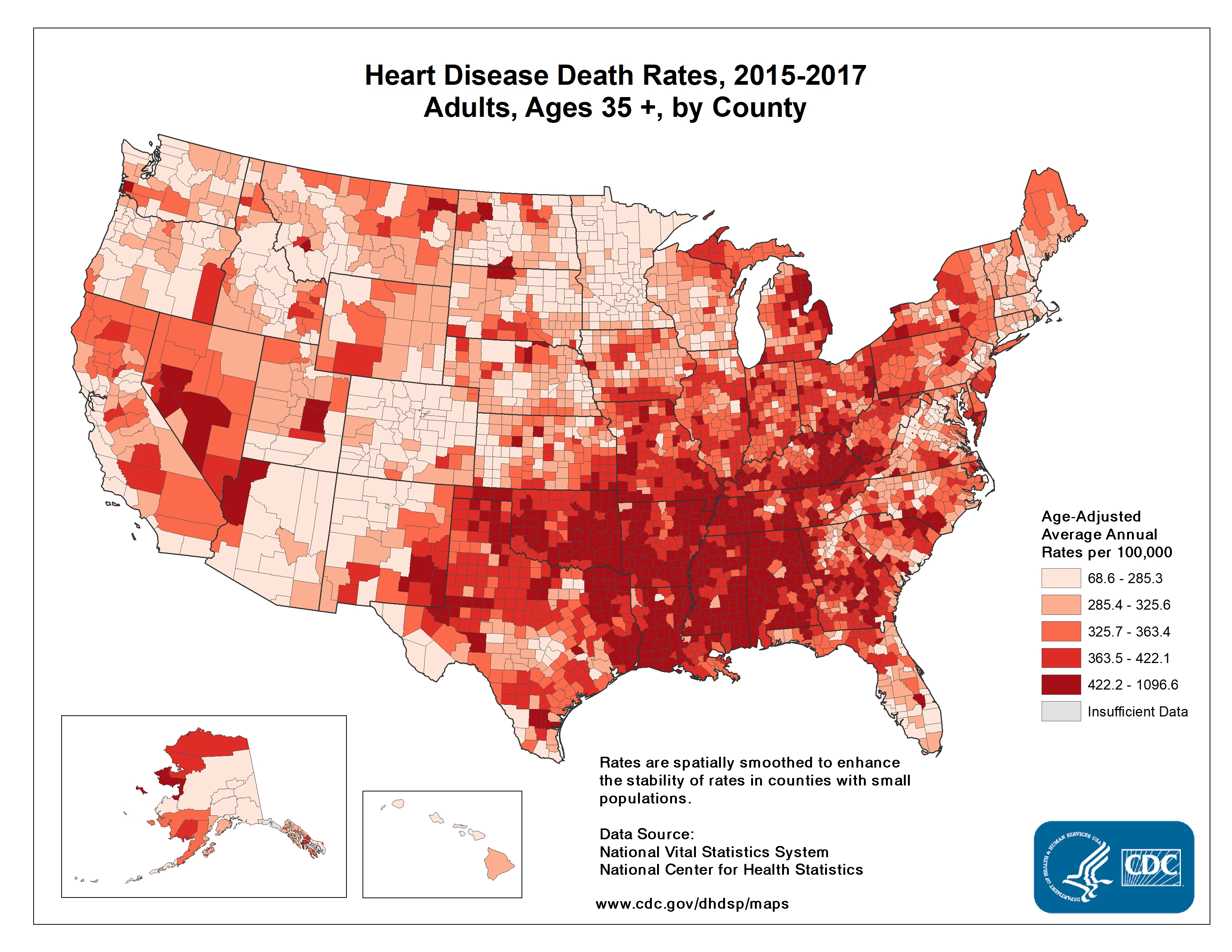
I worry about the effects of COVID-19 on the entire southeastern U.S. which has major health disparities when compared to the rest of the country. The CDC’s 2013 Health Disparities and Inequality Report stated “There are also marked regional diffences, with much lower life expectancy among both white and black Americans who live in the Southeast.” By using human mobility data to monitor the success of social distancing, we see the Southeast is clearly late to the game. The NY Times used anonymous cellphone data to visualize what parts of the U.S. experienced closer to normal travel in late March. Google is generating nice mobility reports. A company called unacast created a social distancing scorecard, shown below on the left. On the right are the CDC’s observed heart disease death rates across the US. These also tend to be highest in the Southeast, often in the same areas of the country who are slow to adopt aggressive social distancing measures. This same trend is seen for other chronic conditions like diabetes. I can tell you now this doesn’t bode well for COVID-19 outcomes. Early data and reporting by The Atlantic already suggests that fatality rates for cases under 70 years of age are higher in the South. Even if you feel removed from the crises in other regions of the U.S., there is likely community transmission of SARS-CoV-2 occurring in your area, and around ~19% of persons infected today will need hospital care in about 10-14 days.
|
|
As you consider ways you can help your own communities, I’d encourage you to consider donating to organizations that help communities of color like supporting businesses owned by minorities. You can support the Detroit Small Business Stabilization Fund here or check out ways to help small businesses in Durham, NC. Consider advocating for equitable aid with your elected officials. Let them know that the NAACP has released resources to guide officials.
Governor Gretchen Whitmer (aka “That Woman from Michigan”) was on The Daily Show with Trevor Noah on April 1. She said 40% of Michigan residents live below the ALICE standards. The Michigan Association of United Ways has an effort, The ALICE Project to help these families. The United Way of Southeastern Michigan serves the counties in Michigan hardest hit by COVID-19 and has a COVID-19 Community Respond Fund (and a pretty good score on Charity Navigator). Finally, if you have the privilege to stay home and avoid becoming sick yourself, you’re helping to save resources and aid for the more vulnerable, the communities we have left susceptible to health disparities for decades.
I have a backlog of scientific papers I’ll summarize next time. For now, here are the News & Views from a quarantined scientist:
The federal Coronavirus task force finally released their projections for estimated deaths in the U.S. from the pandemic: 100,000 to 240,000. You can watch Dr. Tony Fauci explain the fatality predictions on CNN’s State of the Union. Dr. Deborah Birx concurred on the TODAY show. These estimates are from in-house models and the methods were not discussed so cannot be evaluated, but the methods were supposedly influenced by projections made by the University of Washington’s Institute for Health Metrics and Evaluation. You can see the IHME per-state and national projections for bed-days, ICU-days, ventilator days, and deaths in the US. You can read their methods in the pre-print. An in-depth view of the model’s assumptions, including a continuation of strong social distancing measures through June 1, is in this interview. As any good statistican knows, the models are only as good as the assumptions they’re built on. In my home state of North Carolina, as of today, they project 1,534 deaths by August 4, 2020 and a shortage of 213 ICU beds. This is a more favorable projection than that from a few days earlier in the original story by the Raleigh, NC News & Observer.
I’ve noticed that constantly shifting predictions like this may give the general public a sense that scientists and statistical models shouldn’t be trusted, or that “the media” is inflating predictions to stoke panic. The numbers of cases and deaths are a complex function of a lot of factors, and we can estimate them by statistical models. The models are constantly revised as we learn more about the factors (or parameters) that define the models. For example, we can update the case fatality rate as we see what happens in European countries and in the U.S., particularly when health systems are overwhelmed as they are in NYC. As we see the effects of social distancing on viral transmission, the doubling rate of cases can change. Michigan Medicine projects social distancing by 50% of the population changes the current doubling time of 3 days to 7.7 days. This is a good thing—it means the number of cases will now double in a week as opposed to just a few days. All of these factors will continue to change and scientists will continue to update the models based on real-world observations, thereby changing the final projected number of cases and deaths and the associated timeline. The theoretical framework underlying the models is robust and has been developed by scientists, vetted by peer-review, and scrutinized by more scientists. The Washington Post reported the government has worked with a group of about 50 epidemioloists and math modelers at universities over the past decade. These experts have trained all their lives, and many are paid by tax-payer supported biomedical researcher grants. They’re doing the job you’re literally paying them to do…please trust them! The journal Nature published an in-depth special report on epidemiologists’ modelling efforts. The purpose of the models should be to guide policy in an evidence-based way, and to make the best decisions with the information we have at hand now.
A National COVID-19 Convalescent Plasma Project has been launched so that those who have recovered from the disease can register to donate plasma as a potential treatment for current patients (aka convalescent plasma therapy). Early research on a SMALL sample (N=19) in China demonstrated that plasma infusions from recovered patients, which presumably contain pathogen-fighting antibodies, could be effective. This method has been authorized for Compassionate Drug Use, and hopefully proper clinical trials will prove its efficacy. Read the story here.
A digital thermometer company is harnessing big data to view the pandemic. The NY Times reported “In three cities analyzed by Kinsa, simply declaring a state of emergency or limiting the size of public gatherings did not affect the number of people reporting fevers. But closing restaurants and bars and asking people to stay in their homes produced significant results.” Check out Kinsa’s US Health Weather Map.
Researchers have launched a study to examine global attitudes around the pandemic. It takes about 5 minutes, and I would encourage you to take it!
Researchers at Harvard, King’s College London and Zoe Global Ltd, with funding from the UK National Health Service and the Wellcome Trust, launched a mobile COVID Symptom Tracker app which was deployed in the UK on March 24, 2020, garnering over 1 million downloads in just 48 hours. They have just deployed a US version of this app. The data will be securely stored, de-identified and used for aggregate population-level studies. Data from you, even if you are well, can help researchers identify viral hot spots, new symptoms, high risk populations, etc. Please note that this is different from other apps currently available which are symptom screens used to direct people to seek medical care. No medical advice is provided through this app.
You can view view COVID-19 fatality rates per-country over time. Hit play to see how the countries’ rates have changed over time. You can see the grey region of 1-4% is what we are largely seeing for COVID-19. And you can compare this to the case fatality rates of other diseases like SARS (11%). Case fatality rates can be be higher than those actually biologically necessitated by the virus because overwhelmed health care systems will have poorer outcomes.
Speaking of burdened health care systems, a sobering piece about the toll the virus is taking on health care workers.
The US government has extended federal social distancing guidelines to April 30. This was a win in my eyes, despite national grumbling to the contrary, including from an ill-informed law professor who fancies himself an epidemiologist. (Fun fact, research has demonstrated that people who know the least about a topic often believe that they know the most. Read more about the Dunning-Kruger effect here)…
In all seriousness, how to balance the economic downfalls of a shut down with its life saving benefits is an important point of discussion that our leaders should be tackling. The NY Times worked with epidemiologists to create a model illustrating the number of lives at stake across various durations of social distancing. This model is not perfect, but I think the take home lessons are useful. An excerpt:
“Anyone advising the end of social distancing now needs to fully understand what the country will look like if we do that,” cautioned Dr. Tom Inglesby, a health security expert at Johns Hopkins University. “Covid would spread widely, rapidly, terribly, and could kill potentially millions in the year ahead, with huge social and economic impact.”
We can learn a little from Hong Kong, which had very few cases but saw a resurgence upon lifting restrictions. Luckily, expert economic panelists agree (39%) or strongly agree (41%) that abandoning severe lockdowns at a time when the likelihood of infection resurgence remains high (aka now) will lead to greater total economic damage than sustaining lockdown. You can see more professional opinions and added nuances here. For more background, the Initiative on Global Markets (IGM) maintains an Economics Experts Panel (called the IGM Panel for short) comprising leading economists at top United States universities.
Today’s update is a reminder of the lessons from the 1918 Spanish Flu pandemic which killed 50 million people worldwide and around 675,000 in the U.S.
On Friday, May 30, 1919 an article was published in the esteemed journal Science on “The Lessons of the Pandemic” by a Department of Health sanitary engineer George Soper. I can only hope that each and every person who reads this can take the wisdom from 100 years ago to heart. Tell your friends, call your lawmakers, wash your hands. To summarize the piece…
Three main factors stand in the way of prevention:
Public indifference
a. “People do not appreciate the risk they run”
The character of the preventative measures that must be employed
a. “The kind of preventative measures which must be taken in order to control the respiratory infections devolve upon the persons who are already infected”
b. “It does not lie in human nature for a man who thinks he has only a slight cold to shut himself up in rigid isolation as a means of protecting others on the bare chance that his cold may turn out to be a really dangerous infection”
The highly infectious nature of the respiratory infections adds to the difficulty of their control
a. “The period of incubation varies considerably”
b. “The disease may be transmissible before the patient himself is aware that he is attacked”
“There is one and only one way to absolutely prevent it and that is by establishing absolute isolation.”
I fear a scientist could write this same piece in May of 2021. Don’t give her the opportunity. Cancel your plans now. Limit your contacts to your single household now. Self-isolate for 14 days after potential exposure now. The decisions you make today will have impacts on patient counts in 2-3 weeks. You can calculate your pandemic footprint here.
As national hero Dr. Tony Fauci, who has been on the front lines of every infectious disease response since HIV/AIDS says, “I like it when people are thinking I’m overreacting because that means we’re doing it just right.”
Here’s what the scientists are reading.
State by state stats supplied by Johns Hopkins University. Additional stats by The Covid Tracking Project which also assigns a data quality grade to help you interpret how much you should believe the state’s numbers.
Some good news:
Just a quick note today. A story published by many news outlets has headlines that the CDC found coronavirus RNA in the Princess Cruise ship cabins up to 17 days after passengers left. After reading the report from the CDC I would like to emphasize this relevant section:
SARS-CoV-2 RNA was identified on a variety of surfaces in cabins of both symptomatic and asymptomatic infected passengers up to 17 days after cabins were vacated on the Diamond Princess but before disinfection procedures had been conducted (Takuya Yamagishi, National Institute of Infectious Diseases, personal communication, 2020). Although these data cannot be used to determine whether transmission occurred from contaminated surfaces, further study of fomite transmission of SARS-CoV-2 aboard cruise ships is warranted.
Fomite transmission means infection caused by virus or bacteria on a surface. A Harvard epidemiologist has an important Twitter thread regarding the inaccuracy of the headline. Essentially, just because the viral RNA is detectable does not mean the virus is infectious. It is also true that based on this information we can’t completely rule out that the RNA found was in infectious viral particles, so more study is needed.
The study I highlighted in the March 18, 2020 Update looked at fomite transmission, but they actually tested if the viruses could infect cells. They measured the volume of infectious virus present on surfaces and in the air with a metric called TCID50 or 50% tissue culture infectious dose. It quantifies the amount of virus required to infect 50% of tissue culture cells (cells growing in a petri dish). The virus did seem to live as an infectious agent on surfaces like cardboard and plastic from 20-80 hours. Although over time the amount of infectious viral particles exponentially decreased.
Ultimately, we don’t know enough about transmission of the virus from surfaces yet. My advice is that of most public health experts: I would regularly clean surfaces in your home as well as possible, practice good hand hygiene, and not touch your face. If you are in a high risk category, you may consider additional precautions regarding fomite transmission until we know more.
On an optimistic note, a scientist volunteer form has been circulating: “Our plan is to create a national database of scientists located in the United States who are ready and willing to deploy their advanced skills, expertise, and access to reagents/equipment towards the fight against COVID-19 in their local communities.” If you’re a decision maker who wants access to the list, a scientist who wants to sign up, a lab interested in helping, etc. more info is here. As of this morning 6,400 scientists from 49 states, Puerto Rico, and Guam have signed up!
Today’s explainer is a Q&A on COVID-19 testing.
Q: What is the classic COVID-19 test looking for?
A: Every virus has RNA (ribonucleic acid) which allows it to replicate in a host’s cells. A swab is used to sample from your nose/throat and this must be transported to a lab. In the lab, technicians isolate the RNA out of the sample. Then a process called reverse transcription quantitative polymerase chain reaction (RT-qPCR) begins. This 1) turns the viral RNA into complementary DNA (cDNA) 2) amplifies the cDNA. Specifically designed primers that match the viral RNA are used to ensure we are amplifying SARS-CoV-2. You can think of this as two legos that lock together and we can use one lego (the primer) to basically go fishing in a bucket of toys for the matching lego (the virus). Then we use fluorescent dye that binds to DNA and a special sensor in the PCR machine to quantify how much light is emitted—the more DNA, the more light. So a bright fluorescent pattern means DNA matching the virus has been identified and the sample comes from a patient with SARS-CoV-2. A nice explanation of the RT-PCR testing process is here, and it also discusses some of the blunders that have occurred with U.S. testing.
Q: Speaking of testing blunders, what has been going on with U.S. testing?
A: This is more bureaucracy than I would like to go into, but I will point you to some non-scientific sources which contain interviews with scientists that I would consider trustworthy. The NY Times reported on testing blunders here and here. The New Yorker reported on U.S. testing blunders over a week ago. A March 21, 2020 piece by journalists at The Atlantic outlines the testing debacle in the U.S. This article presents a sobering fact about the timeline: “If someone is infected with the coronavirus on Monday, she may start being contagious and infecting other people by Wednesday. But she may not start showing symptoms until Friday—meaning that she was spreading the virus before she even knew she had it. And in some cases, infected people take 14 days to start showing symptoms. The onset of symptoms starts another awful clock. Many people will recover in a few weeks. But if someone’s case is severe, he may not recover for a month. And even if someone’s case is fatal, she may still survive for three weeks. This means that, first, cases discovered now may not become deaths for weeks; second, some people who will die in early April may only start showing symptoms today.”
Q: Is the same test method being used around the world?
A: No! The process I described above is generally the same for each test, but there are different protocols (like a scientific recipe) that can vary slightly but ultimately have the same outcomes. You can think of this as there are many recipes for making an oatmeal cookie. The World Health Organization (WHO) released a test kit using RT-qPCR early on, and is maintaining technical guidance for laboratory testing. Originally the Food and Drug Adminsitration (FDA) only approved the Center for Disease Control (CDC) protocol, but the test kits shipped with a faulty reagent (like an ingredient in a recipe). On February 29, the FDA changed it’s regulations so that any testing lab certified for high-complexity testing could run its own COVID-19 test and bypass the CDC kits.
Starting on page 33 you can see WHO’s February 24, 2020 report on testing in China. They mention serological tests. These are currently being used in Singapore, China, and potentially elsewhere. These tests look for antibodies that a human’s immune system has created to fight the viral infection. So in our metaphor, this is like making a muffin instead of an oatmeal cookie—-completely different receipe but you still get a treat at the end. Read more about Singapore and China. Several U.S. institutions are also working on antibody tests.
Q: Why does testing take up to 48 hours?
A: See the steps involved in the first answer above. The protocol to perform these reactions could take a full day. In addition, technicians may do this at scale by performing the same chemical reaction on hundreds of samples at once using something like a 384 well plate. Waiting for hundreds of samples to be transported from a hospital to a lab environment may be a time-limiting factor. The article from WIRED says “As more labs come online, nearly every step in the RT-PCR test has the potential to run into bottlenecks.” The testing laboratories need PCR instruments that are approved by the CDC and reagent kits from suppliers, lke Qiagen, and some of these are now on backorder.
Q: What is the rapid test we are hearing about?
A: Scientists at Oxford University have created a test that uses RT-qPCR principles but just takes 30 minutes and can be read by the naked eye instead of the PCR machine’s sensor. As of yesterday, a company in the U.S. called Cepheid announced Emergency Use Authorization (EUA) from FDA for a 45 minute test. I can’t find how it works, but it does require an automated GeneXpert System that is already in use around the world. These rapid tests are going to be useful for more widespread surveillance and to solve some of the bottlenecks going on with the classic test in U.S. laboratories.
Q: Should we still be testing?
A: In parts of the country, testing for containment purposes is futile. We can assume the virus is endemic. The strategy is shifting such that testing should be for health care workers and members of high risk populations. I interpret this to mean that if you suspect you could have COVID-19 symptoms but they are mild and you are generally healthy, you should forego the test, assume you have it, and self-quarantine for 14 days. I predict after the initial peak of cases we will move into a testing and containment strategy like we are seeing in countries like South Korea.
Along these lines, Dr. Tony Fauci emphasized the following in the White House Press Briefing on March 21, 2020: Not every single person in the U.S. needs to be tested. Every COVID-19 test requires the use of personal protective equipment (PPE). These materials are high priority for the health care workers who are taking care of people who have COVID-19. Consider this: if you’re going in for testing, you’re taking a gown, mask, and gloves from a health care worker who is trying to save a patient dying in the ICU. My editorialization: You may think this sounds dramatic. It’s not. A hopeful fact: Dr. Fauci expects tests are coming that can be self-administered so a health care worker doesn’t need PPE. When asked about temperature testing instead of viral testing, Dr. Fauci said he doesn’t see a massive distribution of thermometers having an impact on testing.
Q: How accurate are tests?
A: A Michigan Medicine physician at the Town Hall on March 20, 2020 was asked about testing accuracy. She answered that analytically speaking, viral tests are very good at detecting viral particles. The level of detection is down to just a few viral particles. However, it does depend on technique of swab and correct transport. As with any test, false negatives (e.g. test is negative but person is infected) are still possible and they’re treating some patients with negatives but no other explainable cause of disease (e.g. seasonal influenza) as if they have COVID.
News & Views from my rocking chair:
An excellent piece on learning from Singapore and Hong Kong by Dr. Atul Gawande, a trusted author and physician. He says, “The fact that these measures have succeeded in flattening the COVID-19 curve carries some hopeful implications. One is that this coronavirus, even though it appears to be more contagious than the flu, can still be managed by the standard public-health playbook: social distancing, basic hand hygiene and cleaning, targeted isolation and quarantine of the ill and those with high-risk exposure, a surge in health-care capacity (supplies, testing, personnel, wards), and coördinated, unified public communications with clear, transparent, up-to-date guidelines and data.”
A really nice tool to dynamically visualize the classical infectious disease model SEIR (Susceptible–>Exposed–>Infected–>Removed) allows you to estimate your risk exposure on any given day of an epidemic (click the graph to select a day) given the intervention date (click this to slide it) and your close contact with N people. These estimates are based on the reproduction number (number of people the average case infects), incubation period (time between exposure and symptoms), and infectious period (time an infected person can infect someone else). Estimates of these values from the literature are provided in the table.
A data visualization journalist from the Financial Times has been using the Johns Hopkins CSSE data to create these trajectory plots which you may have seen online.
A back of the envelope calculation by a scientist in my field is here. Some of these numbers may be a little off because it is based on estimated parameters (e.g. 20 days between infection and death, 150x cases that we are missing from too little testing), but it’s the correct concept that mattters. With these parameters, 7,500 new deaths will happen in 20 days from March 20, 2020 no matter what we do because 750,000 new infections already occurred on March 20 and ~1% percent of those will die from COVID-19. In other words, the snowball is already rolling down the hill for a subset of the population. Social distancing helps us create a barrier for the snowball farther down the hill (e.g. ~20 days from the start of mitigation measures). We are going to see case and death counts rise until the impact of social distancing measures kick in. Dr. Kellis says: “The only parameter we control is the doubling rate (param3) which is a function of social isolation…So please stay home, stay isolated…” Dr. Tony Fauci said the dynamics of the outbreak are more “robust” in places like Washington and New York. This is why mitigation has been ratcheted up (e.g. true lockdown). If the option is available to you, I would suggest beginning to act like your city is in true lockdown as well and STAY HOME.
First, an important call to action. Personal pleas from health care workers regarding the lack of personal protective equipment (PPE) have me very worried. As do articles by the NY Times and Forbes. While there are contingency strategies from the Food and Drug Administration (FDA), this will not keep our healthcare workers adequately safe. Harvard estimates indicate our hospitals will likely be at capacity or above capacity for months to come—see the figure below. It is unconscionable to not take care of the health professionals at the front lines of critical care. There is a petition you can sign. The Coalition to Protect America’s healthcare has an easy way to send messages. In addition, the American College of Emergency Physicians has a website allowing physicians to easily send an email to elected officials. Based on that, I’ve provided an example script you can adapt for email or use to call your representatives.
Hello, I’m FIRST,LAST and a constituent from TOWN/ZIP. I am reaching out to ask REPRESENTATIVE NAME to provide urgent help for health care workers on the front lines of caring for COVID-19 patients. Emergency physicians and health systems currently face severe shortages of personal protective equipment like N95 masks that will leave many health professionals insufficiently protected in the midst of this outbreak. We need to take action now to fill this gap with every resource we have available, including from the Strategic National Stockpile (SNS). Although the Administration announced that PPE production is ramping up, doctors need these supplies now, and will need significantly more as cases multiply. In order to ensure that emergency physicians and other frontline healthcare providers remain healthy and able to continue to provide vital patient care, the Administration and Congress must exhaust every option available to increase PPE production and prioritize distribution to emergency physicians and other frontline providers. I ask REPESENTATIVE NAME to urge their colleagues and the Administration to immediately address the PPE shortage. Thank you for your hard work answering the phones.
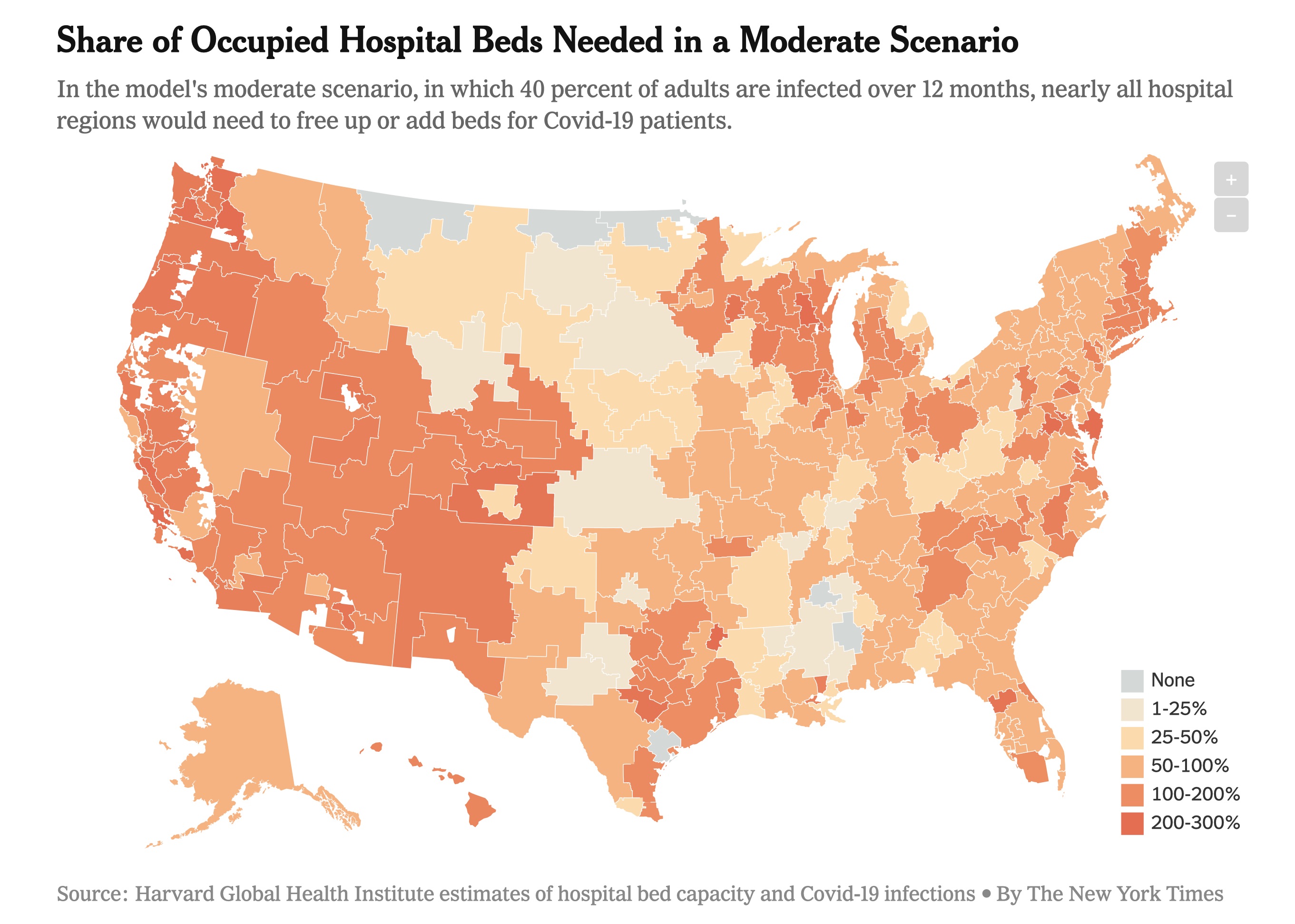
|
If 40% of adults are infected over 12 months our hospitals can barely stay under the threshold of 738,000 hospital beds in the U.S. Hopefully this is a worst-case scenario since the model does not take into account the efforts hospitals can make to quickly increase capacity during an emergency. But based on reports of what is happening to Italy’s health care system, this is what we are trying to avoid.
News & Views from my sofa:
A study published March 19, 2020 provided an updated estimate of the fatality rate of COVID-19 in Wuhan, China as of February 29, 2020. 1.4% (95% confidence interval 0.9%-2.1%) of symptomatic cases died. This is less than initial estimates. However, because of the exponential spread we are seeing outside of China, 1.4% of millions of cases is a lot of deaths.
Johns Hopkins University is hosting a map of confirmed cases, deaths, and recoveries.
An epidemiologist’s blog post explains the reproduction number, R0 or “R naught”, which describes the transmissibility of SARS-CoV-2. I’ve written about R0 previously on the March 16, 2020 update.
Simulations show that undocumented infection facilitates the spread of SARS-CoV-2. By using documented cases, mobility data, and statistical models one study showed 86% (95% confidence interval of 82%-90%) of viral infections were undocumented before China’s January 23 travel restrictions. Undocumented cases are likely not severely symptomatic and therefore shed fewer viral particles. Even though these undocumented cases have a lower transmission rate than that of very sick documented cases, the sheer number of undocumented cases means they are the source of 79% of documented cases. This is more evidence that the identification and isolation of undocumented infections will be necessary to control the outbreak. Also more reason to stay home if at all possible.
I received a question about Gilead and Regeneron’s drug development work that is attracting a lot of investment and media attention. Gilead is in charge of Phase 3 studies for the antiviral remdesivir which I described in the March 20, 2020 Update below. Regeneron Pharmaceuticals and Sanofi have started a clinical program to evaluate a drug call Kevzara. This drug was originally intended to treat patients with rheumatoid arthritis. The drug’s mechanism of action (e.g. the way it works) is by inhibiting the interleukin-6 (IL-6) pathway. This pathway is involved with the inflammatory response of our immune systems. Here is a scientific review if you want to know more, but this science is outside of my area of expertise. Data from China suggests the IL-6 pathway is an important part of the overactive inflammatory response in the lungs of COVID-19 patients. Regeneron also announced a multi-antibody cocktail that may be ready for trials in the summer. More information here. A cautionary note, lots of things have to be considered with therapeutics before we can begin to use them at scale. This includes immediate toxicity, long term effects, and actual efficacy in terms of disarming the virus. Long timelines may seem disheartening, but they mean we won’t rush something to the clinic that does more harm than good.
University of Washington Medicine is sharing resources from their experience with COVID-19 that may be of help to other health care systems beginning to see cases.
Michigan Medicine held a town hall on March 20, 2020. A few points for my local readers.
I want to start with a little explainer on coronaviruses. It’s plural because multiple types exist! We’ve known about them since the 1960s. Coronaviruses usually cause infections in birds and mammals, and were responsible for the severe acute respiratory syndrome (SARS) outbreak in 2003 and the Middle-East respiratory syndrome (MERS) in 2012. The virus SARS-CoV-2 is responsible for the current pandemic, and is a new, or novel, coronavirus. It is called coronavirus because there are crown-like spikes on the virus surface, and corona means crown in Latin (and Spanish, hence the Corona beer logo). These spikes are critical for the virus’ entry into a host cell. Here is info about naming conventions of viruses and their associated diseases. Here is a scientific review article from 2016 on coronaviruses.
An important correction to March 19’s update which I’ve made in the text below. Some evidence shows the O blood group is at a lower risk, not higher risk of COVID-19.
Here are the latest news & views from my home office:
The editorial team at Nature Research has curated relevant scientific articles. The journal Science has curated research, commentary, and news.
The Global Initiative on Sharing All Influenza Data (GISAID) has an incredible tool for visualizing the evolution and spread of the virus from 410 publicly available viral genome sequences. Just like genetic variation happens in people, genetic variation happens in viruses due to mutations. The mutations aren’t usually enough to make the virus survive or infect differently, but it helps us create a phylogenetic tree showing how the viruses are related. The closer they are on the tree, the fewer genetic differences are between them.
This research group’s ‘situation report’ from March 13, 2020 showed the multiple independent introductions of SARS-CoV-2 in the U.S. from travel from China. The clusters of cases in Washington and California that are closely related mean those initial introductions spread in the U.S. via human to human contact. Note, this report is over a week old. They have a nice page for FAQs and Misconceptions too. I want to reiterate there is strong scientific evidence that this virus is of natural origin. The spread of conspiracy theories regarding the virus being purposely manipulated to suit the agenda of a foreign country, political party, or the media is counterproductive and honestly puts lives at risk because people take scientists’ warnings less seriously.
Dr. Francis Collins, the Director of the National Institutes of Health, our nation’s largest biomedical research funder, reiterated the importance of social distancing in his blog today. He always blogs on Tuesday and Thursday about awesome tax-payer supported research, and his blog will have some COVID-19 focus these days.
There is ongoing debate regarding the use of ibuprofen to treat COVID-19 symptoms. National Public Radio (NPR) has a nice review here. A news article from the well-respected British Medical Journal (BMJ) summarizes some of the debate against ibuprofen. As of March 19 the World Health Organization (WHO) does not recommend against the use of ibuprofen. As of now, no solid scientific evidence exists to indicate we should not use ibuprofen to treat COVID-19 symptoms.
STAT is a media company focused on journalism of the life sciences and medicine. I’ve been subscribed to their daily newsletter for years now, and I think they’re a reliable source. They’ve created a guide of the leading efforts for drug and vaccine development. Things in Phase 3 trials are closer to approval for widespread use in humans. The vaccines are all in preclinical stages, which means their approval is likely 12-18 months away.
In terms of therapeutics, I’ve seen buzz about an antiviral called remdesivir. Antivirals fight viral infections by disrupting the virus life cycle so they do not continue to replicate in a host. But antivirals don’t outright kill the viral particles like some antibiotics kill bacteria. A single case study from January (published March 5, 2020) described use of remdesivir and the patient recovered. The authors state, “Although a decision to administer remdesivir for compassionate use was based on the case patient’s worsening clinical status, randomized controlled trials are needed to determine the safety and efficacy of remdesivir and any other investigational agents for treatment of patients with 2019-nCoV infection.” Early work out of China suggested remdesivir and an anti-malarial drug called chloroquine work well in cell-lines (in vitro), but had not been tested in a living organism (in vivo). Over a week ago there were some mixed results about remdesivir, largely due to this pre-print. Remdesvir is now officially in clinical trials, so time will tell. In terms of other drugs, a randomized controlled trial (the gold standard for understanding therapeutic benefit of a treatment) failed for combination therapy of two antivirals in China. You can read the New England Journal of Medicine paper or the NY Times coverage.
Call to Action: The EU Commissioner Thierry Breton is calling on streaming services like Netflix to switch to standard definition to ease the burden on the internet with many persons working from home and video chatting with co-workers, family, and friends. You as a consumer can do your part by switching to standard definition yourself when you start streaming a video. More here.
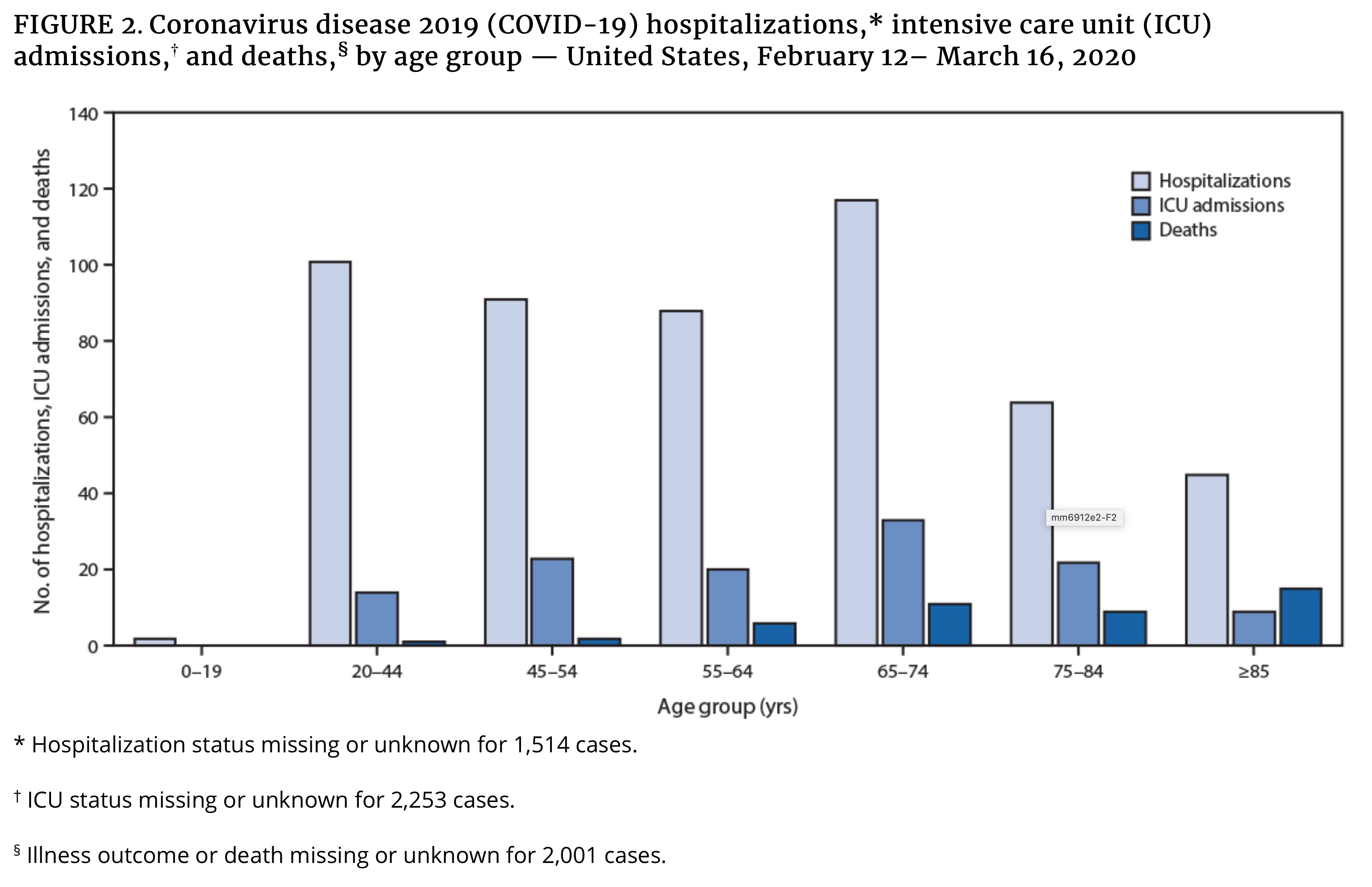
|
A scientist from Seattle has a Twitter thread outlining an approach to combat the U.S. epidemic that may shorten the 18 month time frame now being reported. It starts with a huge roll out of testing to stop the spread that is occurring before symptoms begin. This would be supported with contact tracing by cell-phone location. Serological assays could be used to identify who has recovered from COVID-19 and therefore are likely to possess ongoing immunity. Those individuals with confirmed immunity could the keep economies, companies, and hospitals running. Of the many innovative ideas people are considering, it will be interesting to see what policies actually make it to implementation.
Scientific pre-prints are bringing valuable information to a global force of scientists, policy makers, and informed citizens. A quick description of pre-prints, these publications pass initial screenings by pre-print servers (e.g. medrxiv, biorxiv) but are not peer-reviewed by scientists, an important step to publishing in a respected academic research journal. In other words, they should not be trusted explicitly, but often hold important information. A recent pre-print by Jiao Zhao et al showed that individuals of the A blood group may be at higher risk of COVID-19 when compared to the AB, B, and O groups combined. The odds ratio is 1.21 with a 95% confidence interval of (1.02,1.43). This would mean the odds of COVID-19 are 21% greater in the A blood group compared to the reference group, which in this case is all other blood types. Due to a small-ish sample size of 1,775, some statisticians might say this estimate has a rather large confidence interval. This means we are 95% sure the truth is acually that the odds are anywhere from 2% to 43% greater for A blood group individuals. Note, odds≠probabilty. Conversely, individuals of the O blood group may be at lower risk when compared to A, AB, and B groups combined. The odds ratio is 0.67 with a 95% confidence interval of 0.60-0.75. This means the odds of COVID-19 are 33% less in the O blood group compared to those of other groups. More studies are needed to confirm this in other populations and in a larger sample size, but it could inform clinical guidelines or prioritizaiton of personal protective equipment (PPE) amidst scarcity for health care workers. We are all still at risk of COVID, so this should not change individual behaviors regardless of blood type.
A Chinese charitable organization, Jack Ma Foundation, and the philanthrophic arm of the Alibaba Group released a handbook of COVID-19 Prevention and Treatment aimed at health care workers.
The director of the National Institute of Mental Health released a statement on coping with coronavirus. Here is a collection of mental health resources I’ve seen shared:
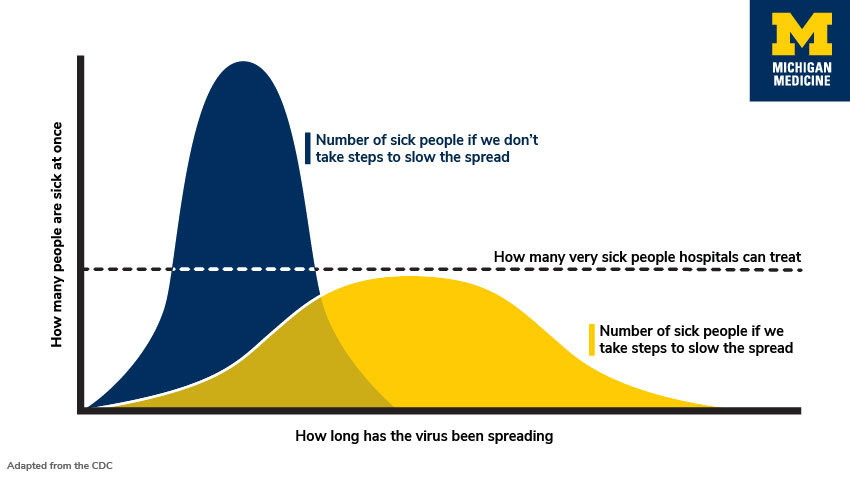
|
It may feel like the world is in chaos. By my assessment, there is no need to panic. However, there is a need to take the COVID-19 outbreak very seriously. Epidemiologists and other health officials are currently advocating for important public health measures which are not a political ploy or a dramatic overreaction. Based on history, peer-reviewed research, and the trajectories of current outbreaks worldwide, we know it is very important that we ‘flatten the curve’ of COVID-19 cases in the United States. This means we slow the virus’ spread now so we won’t overburden a health care system with a finite number of ICU beds, ventilators, and health care professionals. You can read more here and here. You can find scientists’ advice about what social distancing might look like for you here. You can read the CDC’s Community Mitigation Strategies here.
For a variety of reasons, many in society will be unable to practice social distancing adequately in the weeks to come. For example, certain professions such as caregivers and retail workers will need to continue daily operations. If you have the ability to work from home and/or minimize interactions outside your immediate families, please do so now! For many of us this means missing social gatherings or important events which we have planned for, spent money on, or looked forward to for some time. But, this also means we won’t be taking up health care resources for the more vulnerable among us. It also means we can play a role in stopping the exponential spread of the virus. You can learn more about the exponential spread of the virus here. And here are some informative simulations to visualize the positive impact of social distancing.
Importantly, research is emerging that COVID-19 is being spread before carriers are symptomatic, meaning that it’s not enough to just stay home from activities if you aren’t feeling well. Read the scientific pre-print or a more accessible summary. Although, as always, staying home when sick, washing your hands properly, and not touching your face are important public health measures.
It needs to be reiterated that COVID-19 is not the seasonal flu. The summary of a report from the Chinese Center for Disease Control and Prevention found a 2.3% case fatality rate in COVID-19 cases through February 11, 2020. A scientific pre-print attempting to adjust for a variety of data collection biases found an overall case fatality rate of 1.6%. Here is a summary of that work and its limitations. While the estimates thus far are not perfect, the case fatality rate does seem to be higher than that of the seasonal flu which was 0.1% in the U.S. in 2018-2019. Populations with higher co-morbidities (e.g. obesity, smoking), an older population, or an overburdened health care system could see case fatality rates that are higher.
Finally, it is also important to combat misinformation. Before sharing on social media, check the credentials of authors, potential biases of the sources, and the date of the news/posts to ascertain credibility. Memes are not credible. As a point of reference, I believe statements made by U.S. health care officials such as Dr. Tony Fauci, Dr. Deborah Birx, or Dr. Francis Collins are likely to be trustworthy and measured. I cannot vouch for them all, but these Twitter accounts may also be good sources of scientific evidence. The work by Our World in Data is also very thorough and the authors are up front about the limitations to their data analysis.
I will be updating this with useful links in the days to come. Stay well and practice social distancing!
First, here is a data-rich article suggesting that countries that act fast reduce the number of deaths by at least 10x, a real time COVID-19 tracker in US and Canada, and a model hospitals are using to predict the COVID-19 impact and prepare themselves.
Respected biostatisticians, including Dr. Xihong Lin, have been working to analyze 25,000+ lab-confirmed COVID-19 cases from Wuhan, China. Their findings are in a scientific pre-print, summarized with this Twitter thread, and this slidedeck.
In this study, scientists estimated R, the effective reproductive number of the virus. This is the measurement of transmission potential and represents the average number of secondary infections produced by a typical case in a population where some people are susceptible and some are not (e.g. immunity due to previous COVID-19 infection). When R>1 the number of new cases will increase and when R<1 the number of new cases will decrease. Scientists tracked R across time and noted when specific interventions were mandated by the Chinese government. In Wuhan from January 1-10, R was estimated to be 3.88. Afer traffic bans, social distancing, and home quarantine, R was brought down to 1.25 by January 23-February 1. But this was still not enough to cause a decrease in the number of new cases. After centralized quarantine measures began, R decreased to 0.32 in the period after February 2. This R value is finally less than 1 and indicates a decrease in new cases. Centralized quarantine means suspected cases, close contacts of suspected cases, and cases who tested positive are all quarantined in designated spots such as hotels. They continue to receive care, and severe cases can be transported to hospitals’ ICUs. Based on these findings I believe we need to be prepared for such containment strategies down the line and take immediate mitigation (e.g. social distancing) strategies seriously.
Statistical modelling estimates that 60% of infected cases are not ascertained (e.g. not found and contained via quarantine) partially due to being asymptomatic. For example, a study estimated that 17.9% of positive cases on the Princess Cruise ship were asymptomatic, and we are 95% sure the true percentage of asymptomatic cases is between 15.5% and 20.2%. To find these unascertained cases we need more way more COVID-19 testing in the U.S. It is even more imperative that we stay home as much as possible, even if we feel fine. When you do so, you are protecting vulnerable populations including the elderly, our hero health care workers, and others who don’t have the privilege to remain at home.
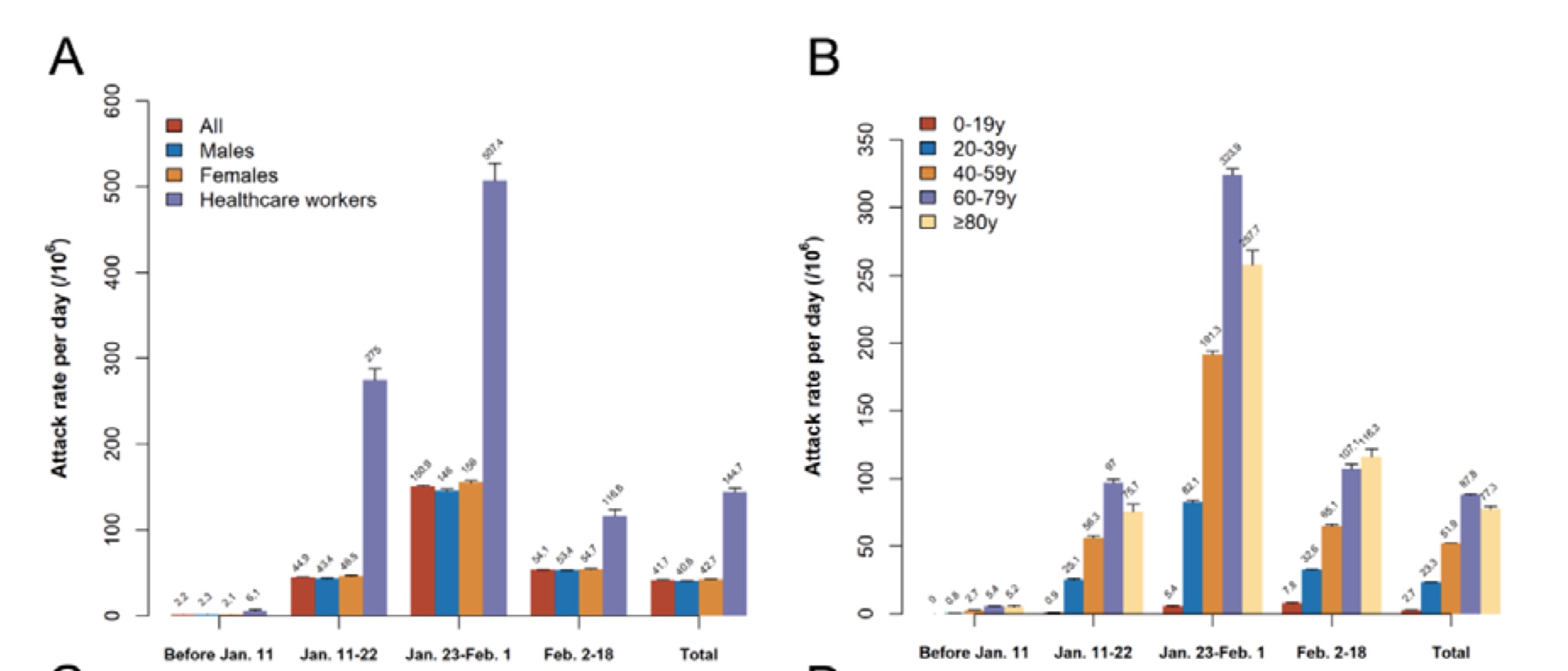
|
Panels A and B of Figure 3 from Wang et al showing the attack rate or number of new cases per day per 1 million people. Notably, health care workers (on the left in purple) and ages 60-79 (on the high in purple) had the highest rates. In the period afer centralized quarantine on February 2 the attack rate dropped for all groups.
Epidemiologists in the UK released a sobering report yesterday regarding the pandemic’s trajectories given non pharmaceutical interventions (e.g. quarantine instead of medicine) in the US and UK. Suppression strategies would reduce R to be < 1 (remember R is the virus’ reproductive number) to < 1, but these strategies would need to be maintained until a vaccine becomes available. Mitigation strategies would reduce R, but not to the desired value of <1, while population immunity builds due to individuals recovering from the virus. Doing nothing in the face of this epidemic could result in 2.2 million deaths in the US. To put this in perspective, the CDC estimates 2.8 million people died of normally occuring disease/accidents in 2017.
The authors make several important points in the Discussion (page 14), which I recommend you read for yourself.
I would like to remind readers that this is one report based on current information and understanding. There is no need to panic, but the findings most likely represent an upper bound on the projected impact of the pandemic. New treatments, scientific understanding of the virus, or innovative solutions may change projections for the better.
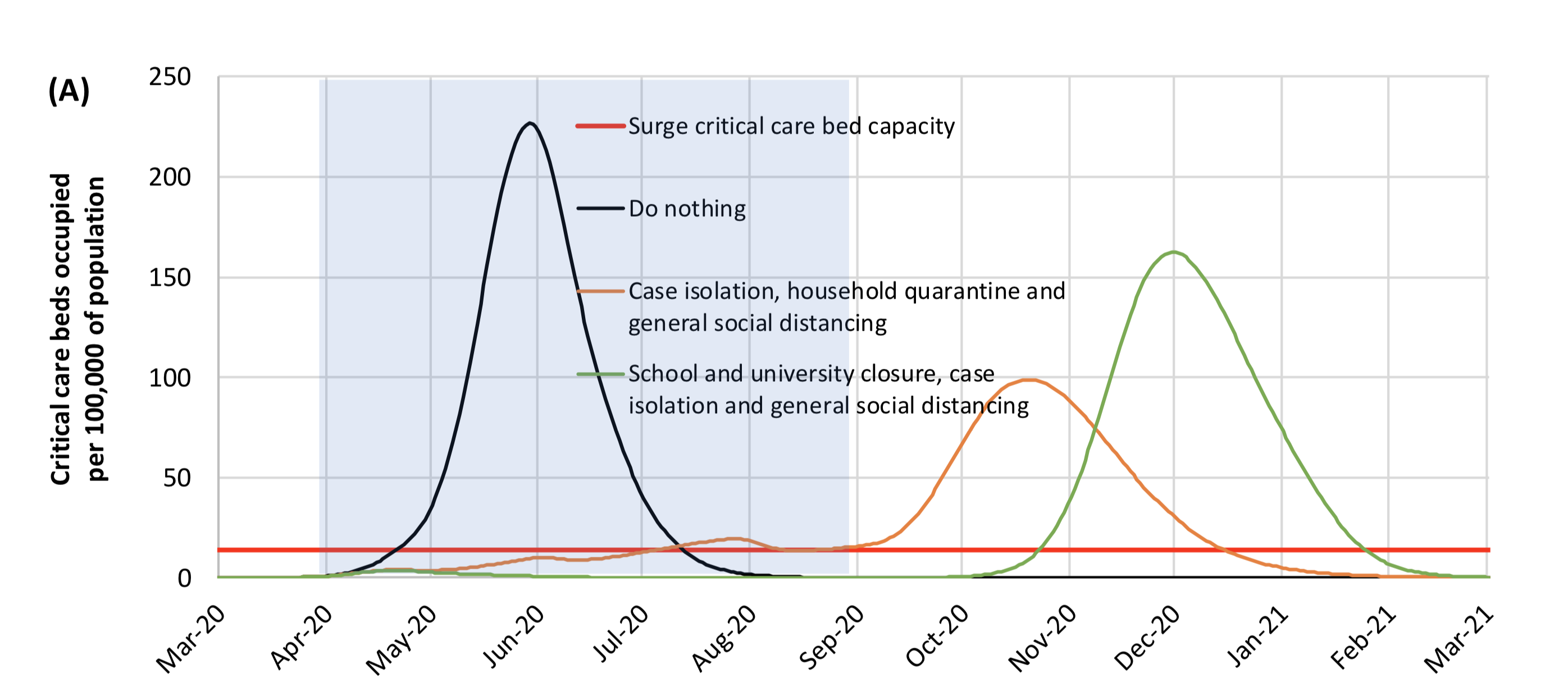
|
Appendix Figure A1 shows ICU bed occupancy in the U.S. under various suppression strategies. The blue shading is 5 months within which the suppression measures are in effect. As you see, the case load would increase when suppression strategies cease.
A few brief updates.
An interview with NIH Director Dr. Francis Collins nicely explained the exponential curve of cases and the civic duty of social distancing.
More sobering projections regarding the length of time required to flatten the curve to minimize overburdening the health care system. Encouragingly, I’ve heard from a resident physician of changes being made in her own hospital to utilize telemedicine and outpatient services to prepare for an influx of patients. Therefore, the “beds for other patients” seen in the second figure is hopefully going to be a smaller number than models are currently accounting for.
A Nature Medicine publication clearly showed the SARS-CoV-2 (the name of the virus) which causes COVID-19 (the name of the novel penumonia trait associated with infection) is not a lab construct or a purposefully manipulated virus. This is important scientific evidence to fight misinformation, the blame game, and xenophobia.
A New England Journal of Medicine publication described the stability of the virus on surfaces and in the air. Based on observations, the virus is predicted to decay over time such that it reaches the limit of detection in 40 hours on copper, 20 hours on cardboard, 60 hours on stainless steel, and 80 hours on plastic. The amount of viable (e.g. infectious) virus on the surface decreases exponentially over time. The virus lasts in the air for at least three hours, but more work is needed to look at time scales past this short window. One potential limitaiton is the ability to perfectly mimic the conditions that would occur when a COVID-19 case coughs.
On a positive note, scientists around the world are looking for ways to help. I know there is an international group that is rapidly mobilizing existing resources to enable the study the genetics of infected patients in the hopes of identifying risk increasing or protective genetic alleles as well as genetic/risk factors correlated with worse outcomes.
A Call to Action, GIVE BLOOD! the American Red Cross is currently only shipping 75% of hospital’s orders due to a national blood shortage. I called yesterday to ask about their precautions and received the following message which NPR reported as well. *“The Red Cross says it has put new measures in place, including checking the temperature of staff and donors before they enter a drive location. Hand sanitizer is provided and used throughout the donation process. Beds are spaced in accordance with social distancing guidelines. And even more attention is given to disinfecting surfaces and equipment.**